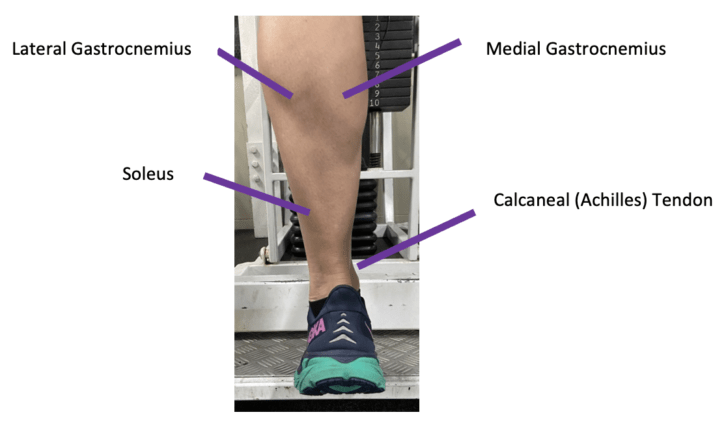

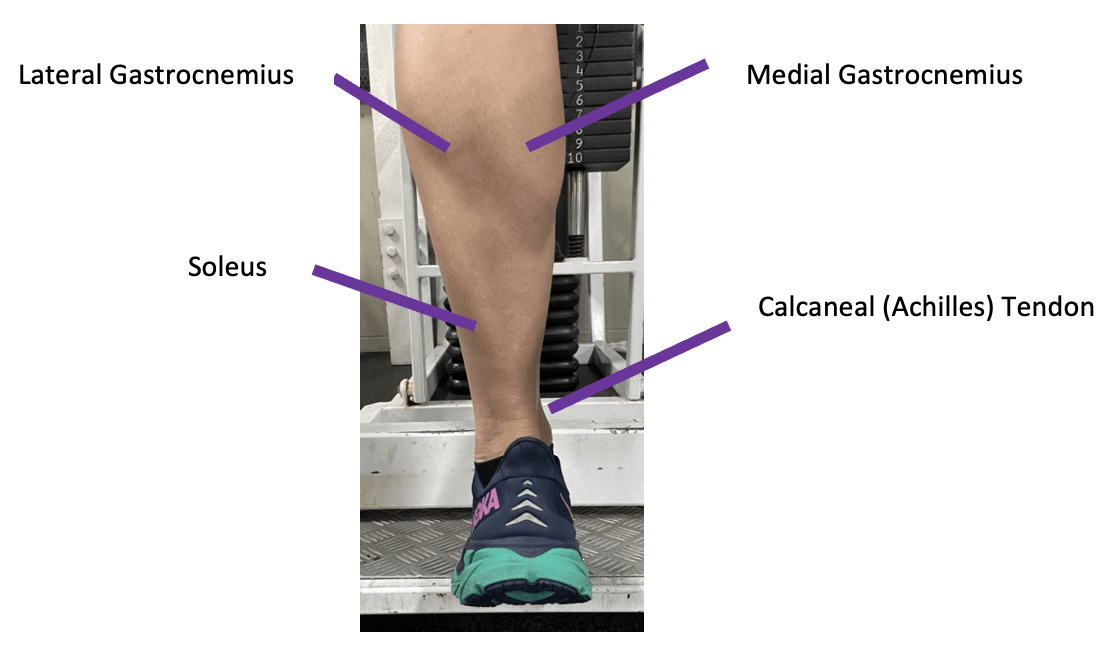
The Achilles is the largest and thickest tendon in the body. It is made up of Type 1 collagen fibres, tenocytes, and proteoglycans which are responsible for the tendon’s tensile strength. These complex interwoven fibres merge from the calf muscles, gastrocnemius and soleus to form the tendon that inserts into the heel bone, the calcaneus. The Achilles is involved in 93% of the plantar force in flexion of the foot. When healthy, this tendon can handle up to nine times the body weight and has a pivotal function in transmitting forces, such as explosive power and control of movements.
When this tendon surpasses its load capacity, it is susceptible to injuries in areas where it compresses around the bone, such as at the bottom of the heel or around the mid-portion above the heel. Overload can be a rapid increase in training volume, intensity, lack of training variation, or change in training surfaces such as hills or weight gain. Achilles tendinopathy can occur in males and females and is most prevalent within the running population. It can also come from sports that involve repetitive jumping movements such as tennis, basketball, and dance. Furthermore, a sustained period away from usual training or absence from any activity can reduce tendon tolerance. The quantity, intensity and frequency of load tolerance are unknown and differ from person to person.
Achilles tendinopathy is where the tendon experiences microscopic degeneration from overuse or ageing. It can develop into a chronic problem if treatment is not initiated in a timely matter. The sooner it can be assessed by a physiotherapist, the better outcomes to return to previous activities.
Symptoms of Achilles Tendinopathy
The main symptoms include pain, morning stiffness and loss of strength around the affected tendon. Pain and stiffness tend to develop gradually and are usually worse first thing in the morning. Runners may notice pain at the beginning of the run which increases after they stop running. The Achilles can be painful on palpation, feel warm, or have a swollen lump around the heel where the calcaneal bursae is located. The relationship between the structure, pain and function of tendons is not fully understood, which contributes to the complexity of managing tendinopathy.
Risk Factors for an Achilles Injury
Risk factors such as gender (males > females), age (>30yrs), obesity, diabetes, changes in hormone levels, poor lower limb muscle control, steroid exposure such as fluoroquinolones, foot alignment, and ankle stiffness can be contributing factors to tendon degeneration. Many of these factors can be modified, such as footwear, general health, sleep patterns, and tendon load.
The Four Phases of the Tendon Continuum
The table below explains the different phases of Achilles tendon injury. Reducing load may allow the tendon to return to the previous stages on the continuum. Identifying this phase can help identify the entry point of rehabilitation and how much activity can be performed to balance activity levels.
| Phase | Name | Tendon change | Prognosis | Healing Time |
| 1 | Reactive Tendinopathy | Normal tissue adaptation in tendon thickness where the load is optimised | Excellent: No or minimal treatment is required. Minimum load modification | Days |
| 2 | Tendon Disrepair | Load rate > remodelling rate. Increased vascularisation to aid tendon repair | Moderate: Good Tendinopathy rehabilitation program | Weeks |
| 3 | Degenerative Tendinopathy | Load rate > remodelling rate and cell loss occurs from excessive load and individual factors and can become degenerative | Good: A moderate tendinopathy rehabilitation program | Months |
| 4 | Tendon Tear/Rupture | Complete tendon tissue breakdown | Possible loss of function. Requires comprehensive rehab program or surgery. | Months+ |
Tendons can move up and down this continuum and this can be achieved through adding and removing load to the tendon, especially in the early stages of tendinopathy such as in Phase 1 and 2.
Treatment Options
- Rest:
In the acute stages of tendinopathy, a short period of relative rest or de-loading may facilitate healing.
- Strengthening:
Your physiotherapist can prescribe specific loading exercises. This approach has some of the strongest evidence supporting its effectiveness in tendon repair.
- Heel wedges:
A heel wedge can be inserted into the shoe to minimise stress on the Achilles tendon.
- Massage:
Release work applied to gastrocnemius and soleus muscles may help pain relief and reduce stiffness.
- Shockwave therapy:
Shockwave therapy can be extremely effective when combined with eccentric loading exercises.
- Heat / ice:
These can be used as adjunct for pain relief.
- Cortisone injections:
Should not be the first approach due to the increased incidence of Achilles tendon rupture after cortisone injections.
- Anti-inflammatory medications:
Pain and possible swelling of Achilles tendinopathy can be improved with non-steroidal anti-inflammatory drugs (NSAIDs) which can be purchased over the counter at your pharmacy.
Management of Achilles Tendinopathy
Achilles Tendinopathy treatment can vary based on irritability and presentation. It is essential to recognise which phase of the tendon continuum applies to ensure that the appropriate exercises are prescribed by your physiotherapist. In addition, they are highly skilled in exercise prescription and guide a person towards a return to sport or activities by finding the “sweet spot” in tendon and training load.
There is substantial research evidence that exercise and load management are critical of tendinopathy rehabilitation. For example, it might be essential to reduce load initially and build tendon tolerance. These exercises may be in the form of isometric exercises, eccentric, concentric and an eventual progression to plyometric load to increase power.
Your pain is a sign of sensitivity. We want this sensitivity to settle, and staying active at the right level can help this.
Your physiotherapist will guide you to make sure you have adequate kinetic chain efficiency such as calf capacity, quadriceps, posterior chain strength, and adequate ankle and great toe range of motion.

Reducing Load
There is some evidence to support several options to reduce Achilles tendon load. One option is to include a rocker shoe or insert a lift to create a higher heel to toe drop. Orthoses can be an option to provide arch support or heel lift. There is some mild evidence that gait retraining where a runner increases step rate by 5-10% can reduce Achilles load. Training changes where volume, frequency or intensity is reduced based on symptoms. These options should be used individually to cater to specific needs.
The Three Phases of Rehabilitation
Phase 1: Calm it down!
It’s essential to modify and reduce painful activities like using a bike, walking, or swimming to reduce tendon load.
Phase 2: Strengthen
Build your kinetic chain such as calf muscle strength which can stimulate the tendon to become stronger. Other muscles of the chain include quadriceps, gluteals and hamstring muscles.
Phase 3: Rebuild
Once symptoms have settled, your physiotherapist will guide you to gradually rebuild your running tolerance by adding distance, frequency and intensity.
Barriers to recovery
It’s important to recognise attitudes and beliefs, behaviours and other environmental factors that may affect recovery. For example, it is easy to catastrophise or have a fear of re-injury that can slow down healing. Having setback are a normal part of the process.
Some may see improvements in a few weeks, and others a little longer. So it’s important to give 8-12 weeks of adequate rehabilitation to see progress. You may have had your symptoms for weeks, months or even years. With time and consistency, you will get there!
Differential Diagnosis
Some other conditions that may present similarly and need to be differentiated from Achilles tendinopathy are:
- Achilles rupture
- Plantaris muscle involvement
- Retrocalcaneal Bursitis
- Plantar Fasciitis
References:
Rio E, Kidgell D, Purdam C, Gaida J, et al. Isometric exercise induces analgesia and reduces inhibition in patellar tendinopathy. Br J Sports Med. 2015 May 15: bjsports-2014
Kaiser BM, Milz KE. Structure-function relationships in tendons: a review. J of Ana 2008;212:211-228
Cook JL, Rio E, Purdam CR, Docking SI. Revisiting the continuum model of tendon pathology: what is its merit in clinical practice and research? BJSM. 2016;50:1187-91
Magnussen R, Warrant R, Thompson B. Nonoperative Treatment of Midportion Achilles Tendinopathy: A Systematic Review. Clin J Sports Med. 2009;19(1):54-64