Cervical radiculopathy, often referred to as a “pinched nerve” in the neck, occurs when a nerve in the cervical spine becomes compressed or irritated as it exits the spinal cord. These nerves travel from the neck into the shoulder, arm, and hand, supplying sensation and muscle control. When a nerve is compromised, it can lead to pain, weakness, numbness, or tingling that radiates from the neck down the arm.
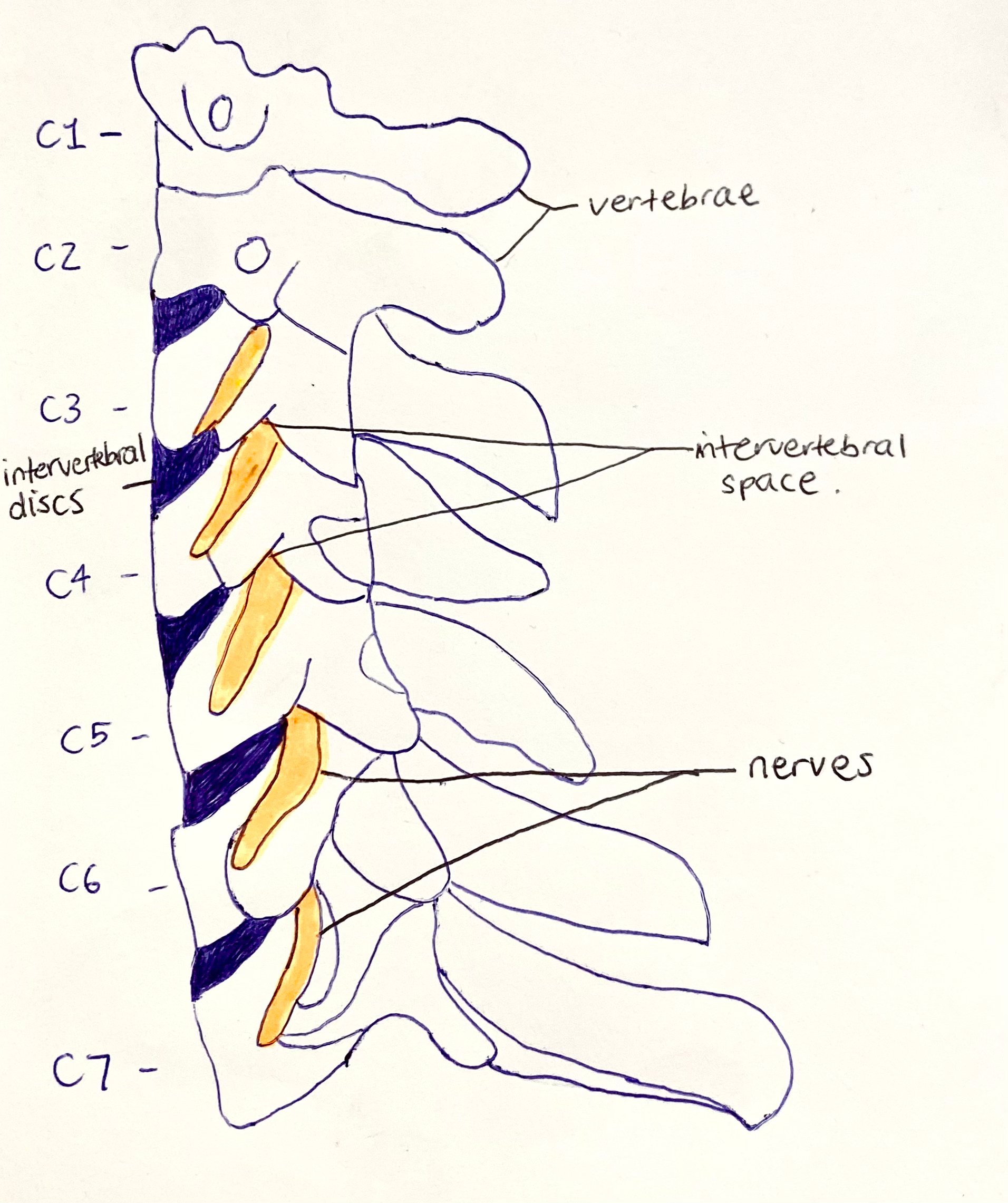
The nerves exit the spinal cord through the intervertebral space, which is the gap between adjacent vertebrae. Between these vertebrae sit the intervertebral discs, which act as shock absorbers and allow movement. Changes to these structures, such as disc herniation, degeneration, or bone spur formation, can reduce space and place pressure on the nerve root.
Cervical radiculopathy can feel frightening due to the spread of symptoms into the arm or hand, but in most cases it is not dangerous and responds very well to physiotherapy for cervical radiculopathy. Understanding the condition is key to managing symptoms effectively, maintaining activity, and preventing long-term complications.
Key Facts
- Cervical radiculopathy affects approximately 83 per 100,000 people annually, with incidence increasing with age.
- More than 85 percent of acute cervical radiculopathy cases resolve without surgery within 8 to 12 weeks.
- MRI findings of disc bulges or nerve compression are common in people without symptoms, highlighting the importance of clinical assessment.
Risk Factors
- Increasing age
- Previous neck injuries
- Poor posture or prolonged screen use
- Repetitive neck or overhead work
- Smoking
Symptoms
- Neck pain that may worsen with movement
- Pain radiating into the shoulder, arm, or hand
- Pins and needles in the arm or fingers
- Numbness in specific areas of the upper limb
- Muscle weakness in the shoulder, arm, or hand
- Reduced grip strength
- Weakened deep tendon reflexes
Aggravating Factors
- Sustained neck positions such as desk or phone use
- Looking up or rotating the neck
- Prolonged driving
- Sleeping in poor neck positions
- Repetitive overhead activities
Causes
There are many causes of cervical radiculopathy, all of which involve pressure on or irritation of a spinal nerve root.
Research by Magnus et al. (2024) identified age-related trends in the most common causes:
In people under 50 years of age, cervical radiculopathy is most commonly caused by disc herniation or trauma. A disc protrusion can narrow the intervertebral space and directly impinge on the nerve root as it exits the spine.
In people over 50 years of age, the most common cause is disc degeneration, also known as cervical spondylosis. As part of normal ageing, discs lose water content and height. In response, the body may form additional bone, called osteophytes or bone spurs, to provide stability. These changes can narrow the nerve exit space, a process known as foraminal stenosis, leading to nerve compression.
Physiotherapists assess how these structural changes interact with posture, movement, and muscle control to determine why symptoms are occurring and how best to treat them.
How Is It Diagnosed?
Diagnosis of cervical radiculopathy involves a combination of clinical history, physical examination, and specific tests performed by a physiotherapist.
Your physiotherapist will assess neck movement, posture, strength, sensation, and reflexes. Special tests may be used to reproduce or relieve symptoms by altering nerve tension or spinal position. This helps identify which nerve root may be involved and whether symptoms are mechanical and movement-related.
Physiotherapists are also trained to identify signs that require referral for further medical investigation, such as progressive neurological weakness or symptoms suggesting spinal cord involvement.
Investigations & Imaging
- MRI
- Provides detailed images of discs, nerve roots, and joint spaces, helping identify disc herniation or foraminal narrowing
- EMG
- Measures muscle electrical activity to confirm nerve involvement or muscle denervation
- Nerve Block
- Helps identify the symptomatic nerve root while providing temporary pain relief
Physiotherapy Management
Exercise
Cervical radiculopathy physiotherapy exercises focus on restoring neck and upper limb movement while reducing neural tension. Early exercises may include gentle neck mobility and nerve gliding techniques to reduce irritation. As symptoms improve, strengthening of the deep neck flexors, shoulder stabilisers, and upper back muscles is introduced to support spinal load and reduce recurrence risk.
Activity Modification
Physiotherapists guide temporary modification of aggravating activities rather than complete rest. This may include limiting prolonged neck positions, adjusting work tasks, and pacing activities to prevent flare-ups while maintaining function.
Manual Therapy
Manual therapy plays a significant role in cervical radiculopathy rehab. Techniques may include joint mobilisation to improve spinal mechanics, soft tissue therapy to reduce muscle guarding, and traction-based techniques to reduce nerve root compression. These interventions are selected based on assessment findings and symptom response.
Postural Retraining
Poor posture can increase neural tension and joint loading in the cervical spine. Physiotherapists provide postural retraining for sitting, standing, and sleeping to reduce stress on the affected nerve root and support long-term recovery.
Bracing & Taping
Rigid bracing is rarely required. Taping may be used short term to provide postural feedback and reduce protective muscle guarding during movement.
Dry Needling
Dry needling may be used to address secondary muscle spasm in the neck and shoulder region that develops in response to nerve irritation. This can improve comfort and movement tolerance.
Heat & Ice
Heat may assist with muscle tension, while ice may help reduce pain in acute flare-ups. Physiotherapists advise appropriate use based on symptom presentation.
Tens
TENS may be used as a short-term pain modulation tool to assist with exercise participation and daily activities.
Education
Education is central to physiotherapy for cervical radiculopathy. Physiotherapists explain nerve pain, reassure patients about favourable outcomes, and address fear of movement. Understanding that symptoms do not equal damage is critical for recovery.
Other
Breathing strategies, sleep advice, and stress management may be included when muscle tension or poor recovery patterns are contributing to symptoms.
Other Treatments
Corticosteroid injections may be used as an adjunct in more severe cases. These injections aim to reduce inflammation and pain around the nerve root, allowing improved participation in cervical radiculopathy physiotherapy.
Surgery
Surgery is generally considered only when conservative treatment, including physiotherapy, has not been successful after at least six weeks, or when there are significant or worsening neurological deficits.
Common surgical options include anterior cervical discectomy and fusion, posterior cervical foraminotomy, and cervical disc arthroplasty. Physiotherapy remains essential both before and after surgery to optimise outcomes.
Prognosis & Return to Activity
The prognosis for cervical radiculopathy is generally very good. Most acute cases improve significantly within 8 to 12 weeks without surgery. Physiotherapy accelerates recovery by restoring movement confidence, strength, and neural mobility.
Return to work and sport is guided gradually, with physiotherapists ensuring activities are resumed safely without provoking nerve irritation.
Complications
- Persistent nerve pain if activity is avoided
- Chronic neck stiffness
- Muscle weakness due to disuse
- Reduced work or activity tolerance
Preventing Recurrence
- Maintain ergonomic workstation setup to reduce cervical nerve loading
- Avoid prolonged sustained neck postures
- Perform regular neck and upper back strengthening exercises
- Manage flare-ups early with physiotherapy input
- Maintain general physical activity to support spinal health
When to See a Physio
- Neck and arm pain lasting more than a few days
- Pins and needles or numbness in the arm or hand
- Muscle weakness or dropping objects
- Recurring episodes of nerve-related neck pain
- Difficulty performing work or daily activities