Constipation is common, but it can be uncomfortable to talk about, even with a health professional. It is not “just a nuisance”. Constipation is a bowel (defecation) disorder that can significantly affect daily life through bloating, pain, reduced appetite, poor sleep, and anxiety about going to the toilet.
Bowel habits vary between individuals. A commonly cited “typical” bowel movement frequency can range from three times per day to three times per week. That means constipation is not simply “not going every day”. Constipation is more about the overall pattern including stool consistency, straining, a feeling of incomplete emptying, and how much effort is required to open your bowels.
Constipation can happen at any age. It can be related to diet, hydration, medications, routine changes, pregnancy, pelvic floor muscle coordination issues, and a wide range of medical conditions. Many people also develop constipation habits over time, such as ignoring the urge to go or routinely rushing on the toilet, which can reduce normal rectal signalling and increase straining.
Physiotherapy for constipation, particularly with a pelvic health physiotherapist, can be very helpful when constipation involves pelvic floor dysfunction (for example dyssynergic defecation, where pelvic floor muscles do not relax properly during opening). Physiotherapists also support toileting posture, breathing techniques, bowel habit retraining, abdominal and pelvic floor coordination, and return to comfortable bowel movements without ongoing straining.
Key Facts
Risk Factors
- Low dietary fibre intake (insufficient stool bulk and softness).
- Low fluid intake (stool can become harder and more difficult to pass).
- Low physical activity and prolonged sitting.
- Pregnancy and postpartum period.
- Pelvic floor dysfunction including dyssynergic defecation (poor relaxation during opening).
- Medication side effects (varies by medication and individual).
- Neurological or metabolic conditions affecting bowel motility.
- History of avoiding bowel urges due to routine, privacy, pain, or past trauma.
Symptoms
- Bowel movements that feel difficult, slow, or require frequent straining.
- Hard or lumpy stool (often Bristol Stool Form Scale type 1 to 2).
- A sensation that the rectum has not emptied fully after a bowel movement.
- A sensation of blockage or obstruction at the anus or rectum.
- Needing to use manual manoeuvres (for example finger assistance or perineal support) to help stool pass.
- Going less often than your usual pattern, especially if accompanied by straining or hard stool.
- Bloating, abdominal discomfort, or feeling “heavy” in the lower abdomen.
Aggravating Factors
- Ignoring the urge to open your bowels and then trying later without a strong urge (reduces normal rectal signalling over time).
- Rushing on the toilet, breath-holding, or straining hard to “get it out”.
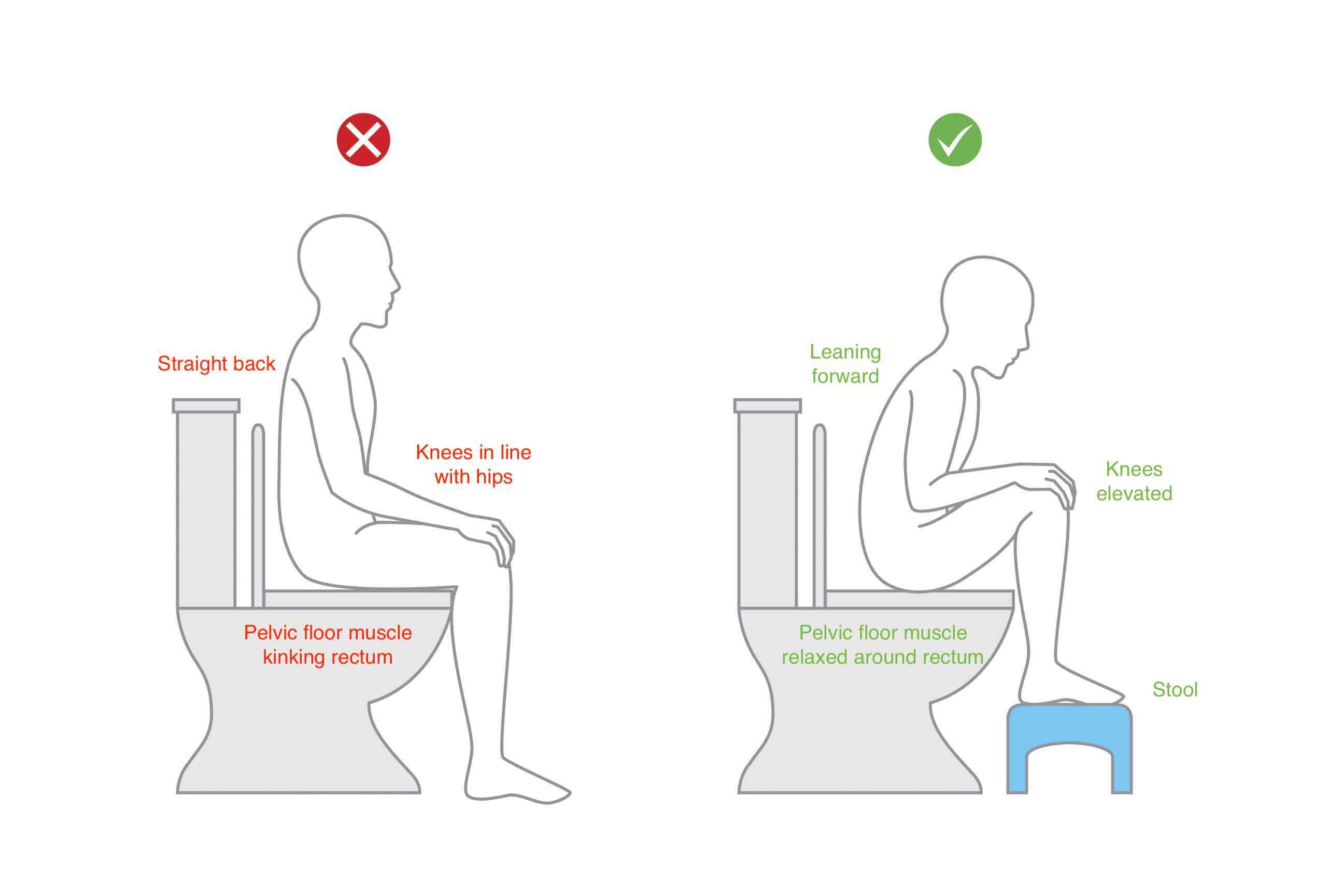
- Sitting with feet flat and knees low (often increases straining compared to a hips-flexed position).
- Low fibre intake, low fluid intake, and reduced movement, particularly during routine changes or travel.
- Pregnancy and postpartum changes (hormones, reduced gut motility, pelvic floor changes, pain, and fear of straining).
- Medications that slow bowel motility (for example some pain medications and other prescriptions, depending on the person).
Causes
Constipation is defined by the International Urogynecological Association (IUGA) as “a complaint that bowel movements are infrequent and/or incomplete and/or there is a need for frequent straining or manual assistance to defecate”. In plain terms, constipation can show up as going less often, needing to strain, passing hard stool, feeling like you did not empty properly, or needing to assist stool to pass.
Constipation has many possible causes. Some are related to bowel motility (how quickly the bowel moves), some are related to stool consistency (often influenced by fluid and fibre), and some are related to pelvic floor muscle coordination. Pelvic floor coordination matters because opening the bowels requires the pelvic floor muscles to relax and lengthen while the abdominal wall creates gentle pressure to move stool out. If pelvic floor muscles tighten or “hold on” during opening (often called dyssynergic defecation), stool can be difficult to pass even if you are eating well and drinking enough.
Common contributing factors include:
- Diet and hydration:
Lower fibre intake can reduce stool bulk and softness. Fluid intake also influences stool consistency. Australia’s Nutrient Reference Values (NRVs) provide Adequate Intake guidance for water and dietary fibre. - Routine, privacy, and time:
People often ignore urges due to busy schedules, limited privacy, or discomfort using public toilets. Over time, ignoring the urge can reduce the rectum’s natural signalling. - Pregnancy:
Hormonal changes can slow gut motility, and there can be fear of straining, pelvic floor changes, and reduced movement. - Medical conditions:
Metabolic disorders, neurological conditions, gastrointestinal disorders, and some cancers can contribute. Psychological stress can also be involved. - Medications:
Some medications can slow the bowel or change stool consistency. A GP review is important when constipation is persistent or new, especially if symptoms are significant or you have red flags.
Because the causes are varied, management works best when it is matched to the main driver for you. This is where pelvic health physiotherapy for constipation and a GP assessment can work together to form a clear, safe pathway.
How Is It Diagnosed?
Constipation is diagnosed based on your symptoms and a clinical assessment. A GP will usually ask about bowel frequency, stool form, straining, incomplete emptying, urgency, abdominal pain, bleeding, unintentional weight loss, diet, fluid intake, medications, pregnancy status, and relevant medical history.
Many clinicians use the Rome IV criteria to describe functional constipation. Rome IV states that functional constipation requires two or more of the following: straining with more than 25% of bowel movements; lumpy or hard stools (Bristol type 1 to 2) with more than 25% of bowel movements; sensation of incomplete evacuation; sensation of blockage; manual manoeuvres; fewer than three spontaneous bowel movements per week; with loose stools rarely present without laxatives and insufficient criteria for irritable bowel syndrome.
If constipation is persistent, severe, new, or associated with red flags, your GP may perform an abdominal and anorectal examination to check for tone, fissures, haemorrhoids, prolapse, masses, or other concerns. They may also review medications and consider investigations if needed. In pelvic health physiotherapy, assessment focuses on toileting habits, breathing and abdominal bracing strategies, and pelvic floor muscle coordination. Where appropriate and with consent, a pelvic floor examination may be used to check whether the muscles can relax for bowel emptying.
It is important to seek medical review urgently if you have blood in stool, persistent vomiting, severe worsening pain, fever, unexplained weight loss, anaemia, a sudden significant change in bowel habits, or a family history of bowel cancer with concerning symptoms.
Investigations & Imaging
- Bristol Stool Form Scale
- Helps describe stool consistency. Types 1-2 are hard/lumpy and commonly associated with constipation.https://www.nice.org.uk/guidance/cg99/resources/cg99-constipation-in-children-and-young-people-bristol-stool-chart-2
- Physical examination
- An abdominal and anorectal exam can assess for fissures, haemorrhoids, tone, masses, strictures, or signs of obstruction.
- Blood tests
- May be used to screen for metabolic contributors (for example thyroid issues) or anaemia when clinically indicated.
- Imaging or colonoscopy
- Used when red flags are present, symptoms are atypical, or obstruction and other pathology must be excluded.
- Anorectal manometry / balloon expulsion testing
- Assesses pelvic floor and rectal coordination when dyssynergic defecation is suspected and symptoms persist.
Grading / Classification
- Functional constipation (Rome IV framework)
- Constipation symptoms meeting Rome IV criteria, without evidence of structural disease explaining symptoms. Often influenced by stool form, habits, and pelvic floor coordination.
- Defecation disorder (dyssynergic defecation)
- A pelvic floor coordination problem where pelvic floor muscles do not relax properly during attempted bowel emptying, making stool hard to pass even with adequate diet and fluids.
- Secondary constipation
- Constipation driven by an identifiable factor such as medication effects, metabolic issues, neurological conditions, pregnancy-related changes, or structural bowel issues.
Physiotherapy Management
Physiotherapy for constipation is most useful when constipation is linked to toileting mechanics, pelvic floor dysfunction, or ongoing straining. Pelvic health physiotherapists assess how you breathe, brace, and coordinate your pelvic floor during bowel emptying, and they teach strategies to reduce strain while improving emptying.
This is not just general advice. If pelvic floor muscles are overactive or poorly coordinated, simply “eat more fibre” may not fix the problem. Physiotherapy focuses on the how of toileting: posture, foot position, pelvic floor relaxation, and abdominal pressure control, plus a plan to build consistent bowel habits that support natural rectal signalling.
In people with dyssynergic defecation, pelvic floor biofeedback-based retraining is widely described as effective. Physiotherapy often works alongside your GP’s management (for example medication review, laxatives when appropriate, and screening for medical causes).
Exercise
Exercise helps constipation for many people by improving overall gut motility and reducing time spent sedentary. For physiotherapy, “exercise” also means specific pelvic floor and abdominal coordination exercises when a defecation disorder is suspected.
If you strain regularly, your pelvic floor may be tight, overactive, or poorly coordinated. A pelvic health physiotherapist can teach relaxation and lengthening strategies for the pelvic floor, combined with diaphragmatic breathing. Later, they may progress to functional core control that supports bowel emptying without breath-holding or pushing down through the pelvic floor.
In some cases, gentle abdominal massage techniques, hip mobility work, and pelvic floor down-training can reduce the “holding” response that blocks emptying. If pelvic floor weakness or prolapse is also present, your physiotherapist will balance relaxation with strength and support strategies, because effective bowel emptying needs both coordination and appropriate closing strength after opening.
Activity Modification
Activity modification for constipation is often about changing daily habits that drive straining and poor signalling. A physiotherapist may guide you to stop doing “just in case” sits on the toilet, stop pushing without an urge, and stop repeatedly ignoring the urge when it appears after meals.
Instead, your plan may include: a consistent routine (often using the natural post-meal gastrocolic reflex), allowing enough time without rushing, and setting up your environment for privacy and comfort. These changes can be especially important for people who avoid public toilets, who have demanding work schedules, or who have developed fear around bowel movements after painful haemorrhoids or fissures.
If constipation is linked to medications or pregnancy, activity modification also includes pacing and gentle movement throughout the day, because prolonged sitting can worsen stool transit.
Manual Therapy
Manual therapy is not a universal treatment for constipation, but it can be appropriate in selected pelvic health physiotherapy cases. If pelvic floor muscles, abdominal wall, hips, or lower back are highly guarded and contributing to poor relaxation and difficulty emptying, hands-on therapy can help reduce muscle tension and improve comfort.
Manual therapy may involve external soft tissue techniques to the abdominal wall, hips, and pelvic region, and in some cases internal pelvic floor techniques (only with informed consent) aimed at reducing overactivity and improving the ability to relax for defecation. Manual techniques should always be paired with active retraining, because lasting improvement depends on learning how to coordinate breathing, pelvic floor relaxation, and abdominal pressure during toileting.
Postural Retraining
Postural retraining is a key physiotherapy component because toileting posture directly changes the angle of the rectum and pelvic floor mechanics. Many people strain simply because their position is not helping stool pass.
A common evidence-informed setup is to raise the feet so the knees are higher than the hips, lean forward with elbows on knees, and keep the belly relaxed. This posture often reduces the need to strain and helps the pelvic floor lengthen.
Your physiotherapist can also correct common problems like sitting bolt upright, clenching buttocks, holding breath, or repeatedly pushing. If you have hip pain, pregnancy-related discomfort, or mobility limits, your physio will adapt posture so it is achievable and safe.
Education
Education is the highest-value part of constipation rehab because small technique changes can reduce straining quickly. Your physiotherapist will usually cover:
- Responding to urge:
If you get a clear urge to open your bowels, trying to go at that time can support normal rectal signalling. Ignoring urges repeatedly can make the signal weaker over time. - Stool form and targets:
Using the Bristol Stool Form Scale can help you identify if stool is too hard (types 1 to 2) or too loose. Hard stool often needs a plan that combines hydration, fibre adjustments, and sometimes medical support. - Fluids and fibre (Australian guidance):
Australia’s NRVs provide Adequate Intake guidance for water and dietary fibre. Your physio can help you implement these changes in a way that does not worsen bloating or discomfort, because increasing fibre too quickly can flare symptoms for some people. - Breathe, brace, bulge technique (defecation mechanics):
Many people hold their breath and strain. Instead, physiotherapy teaches diaphragmatic breathing to relax the upper body, then a gentle abdominal expansion strategy to create pressure without clenching pelvic floor muscles. The goal is a controlled “push” that is directed into the belly, while the pelvic floor relaxes, rather than a hard strain. - Finishing strategy:
After passing stool, learning how to re-engage pelvic floor closure can help some people who experience leakage or a sensation of incomplete closure.
Other
Other supports may include pelvic floor biofeedback retraining (where available), particularly when a defecation disorder is suspected. Biofeedback-based pelvic floor retraining is widely described as effective for dyssynergic defecation.
Your physiotherapist may also coordinate with your GP about medication contributors, safe use of laxatives when appropriate, and escalation when red flags are present. In pregnancy-related constipation, physiotherapy can tailor posture and breathing strategies to suit a growing belly and pelvic floor changes.
Other Treatments
Other treatments are often guided by your GP and may include:
- Medication review:
Adjusting or changing medications that contribute to constipation where appropriate. - Fibre supplementation or laxatives:
Sometimes used short-term or longer-term depending on the cause. These should be used under medical guidance, particularly if you have pain, bleeding, significant bloating, or a history of bowel disease. - Management of contributing conditions:
For example thyroid issues, neurological conditions, pregnancy-related constipation, or gastrointestinal disorders.
Physiotherapy often complements these approaches by reducing straining, improving pelvic floor coordination, and making toileting more effective, which can reduce reliance on ongoing laxatives for some people.
Prognosis & Return to Activity
Prognosis depends on the cause. Constipation driven by routine changes, low fibre, low fluids, or temporary medication effects often improves with targeted lifestyle changes and appropriate medical support.
If constipation is linked to pelvic floor dysfunction (dyssynergic defecation), improvement is still very achievable, but it often requires a structured retraining program rather than simple diet changes alone. Education and pelvic floor biofeedback-based retraining are commonly described as effective for dyssynergic defecation.
Most people do best when they have a combined plan: GP review (to rule out medical causes and guide medications as needed) plus pelvic health physiotherapy (to fix toileting mechanics and reduce straining), plus gradual adjustments to fibre and fluids aligned to Australian NRVs.
Complications
- Haemorrhoids and anal fissures from repeated straining and hard stool.
- Pelvic floor dysfunction worsening over time if pushing and breath-holding becomes habitual.
- Worsening bloating and abdominal discomfort, and increased anxiety around toileting.
- Rectal prolapse risk in severe long-term straining in some people (requires medical assessment).
Preventing Recurrence
- Respond to the bowel urge when it appears (often after meals) rather than repeatedly delaying, to maintain normal rectal signalling.
- Use a foot stool so knees are higher than hips, lean forward, and relax the belly to reduce straining and support pelvic floor relaxation.
- Aim for steady, gradual fibre increases and adequate fluids guided by Australian NRVs, rather than sudden large increases that can worsen bloating.
- Avoid breath-holding and hard pushing. Use diaphragmatic breathing and a gentle abdominal expansion strategy taught by a pelvic health physiotherapist.
When to See a Physio
- If you strain most times you open your bowels, or you regularly feel incompletely emptied.
- If you need manual assistance (splinting, digital evacuation, perineal support) to pass stool.
- If constipation is present alongside pelvic floor symptoms such as prolapse symptoms, urinary issues, or pelvic pain.
- If constipation began or worsened during pregnancy or postpartum and you want a pelvic floor-safe plan.
- If diet and fluid changes have not helped and you suspect pelvic floor coordination may be the issue.