Discogenic low back pain describes low back pain that is thought to be coming primarily from an intervertebral disc (the spinal “shock absorber” that sits between the vertebrae). Discs help your spine move, share load, and absorb forces from bending, lifting, running and sitting. A disc can become painful when it is overloaded, irritated, or sensitised, which can happen with a sudden spike in load (like a big lift or awkward bend), or with repeated or prolonged positions that the disc is not currently conditioned for.
You might also hear discogenic back pain described using other terms such as disc strain, disc overload, disc bulge, disc herniation, or degenerative disc disease. People often use these interchangeably, though they technically mean slightly different things. Importantly, your scan result does not automatically predict how much pain you will have. Many people have disc changes on imaging and have no symptoms at all, and many people recover well without needing a scan, injection, or surgery.
Understanding what might be happening can reduce fear. The spine is not fragile. Discs are tough, strongly attached to the vertebrae, and they do not “slip in and out”. Discogenic pain is best approached by focusing on your symptoms, your function, and your goals. In physiotherapy, we typically manage disc-related presentations by first settling symptoms, then restoring normal movement and confidence, and finally building a resilient back that can handle your work, sport and daily life.
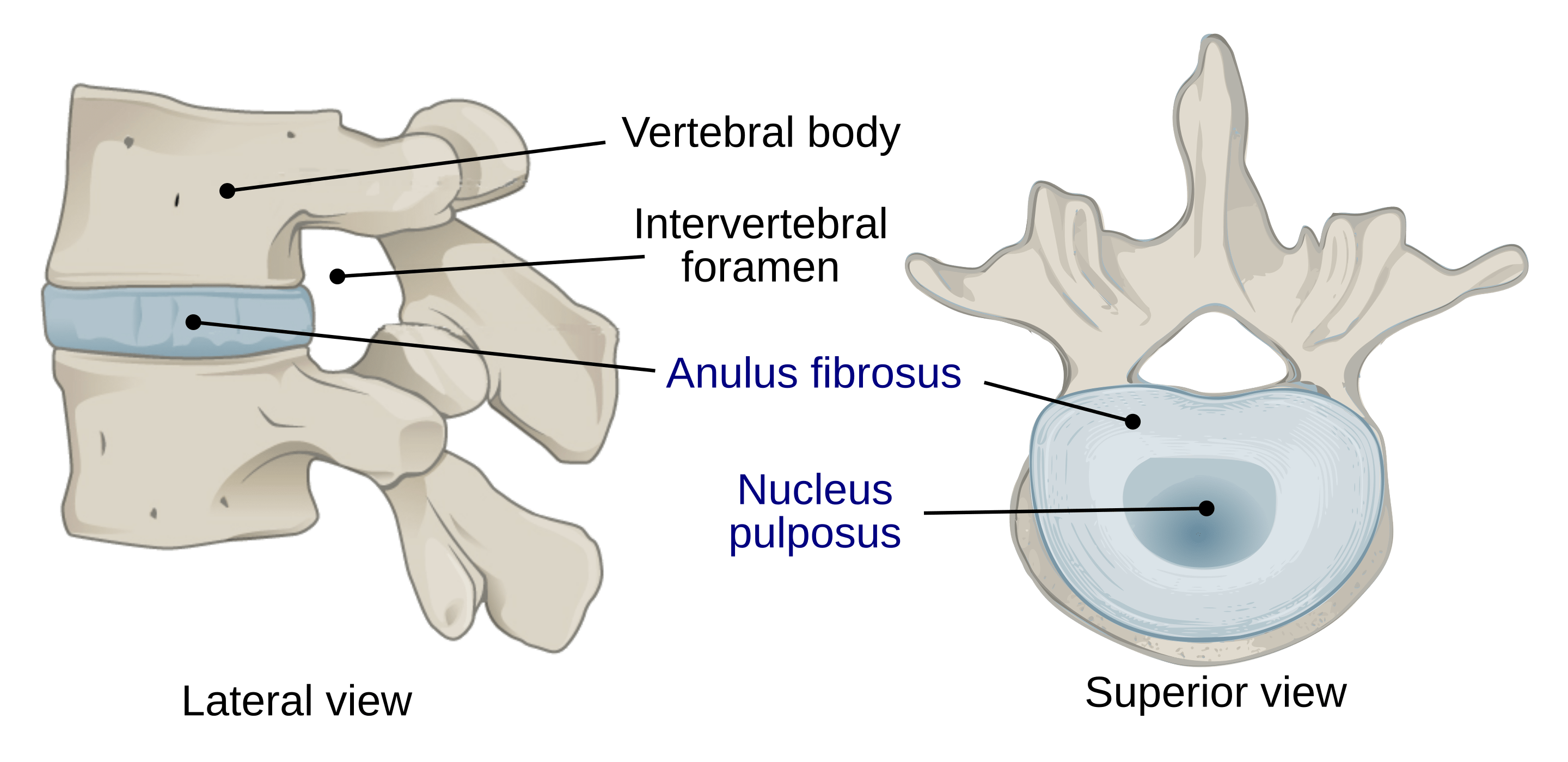
What is a disc made of? A disc has a tough outer ring (the annulus fibrosus) and a more gel-like centre (the nucleus pulposus). A simple way to picture this is a strong tyre-like ring with a softer filling. When you bend forward, pressure within the disc tends to shift toward the back portion of the disc, which can increase symptoms for some people, especially if the disc is already irritated. Other people feel worse with arching their back, prolonged standing, or long sitting. This is why a personalised physiotherapy assessment matters.
Discogenic pain is usually felt in the low back and can refer into the buttock, hip or groin. If nearby nerve roots are irritated (either from chemical inflammation or mechanical pressure), symptoms can extend into the leg and may include pins and needles, numbness, or weakness. Physiotherapy for discogenic low back pain addresses both the disc’s sensitivity and the way your back is being loaded across the day, so you can calm it down and then build it back up safely.
Key Facts
- Imaging findings such as disc degeneration and disc bulges are common even in people without back pain, and the prevalence increases with age. This is one reason routine early imaging is not recommended for uncomplicated low back pain. 🔗
- Most cases of discogenic pain improve with conservative treatment, with 85% of people experiencing full symptom resolution within a few months. 🔗
Risk Factors
- Sudden increase in bending, lifting, or training load (a workload spike)
- Prolonged sitting or driving with limited movement breaks
- Manual work with repeated flexion and lifting, especially when fatigued
- Reduced trunk and hip strength or endurance (lower capacity to tolerate load)
- Poor sleep, stress, or low physical activity levels, which can amplify pain sensitivity and reduce recovery capacity
- Previous episodes of back pain, particularly if return-to-activity was not progressively rebuilt
Symptoms
- Low back pain that may be central or one-sided, often described as deep, aching, sharp, or “caught”
- Pain that may spread into the buttock, hip or groin (referred pain)
- Symptoms worsen with certain postures or loads, commonly bending, sitting, lifting, or repeated flexion (but not always)
- Stiffness and reduced confidence to move, especially after rest or first thing in the morning
- Pain with coughing, sneezing, or straining (due to pressure changes), in some cases
- Leg symptoms if a nerve root is irritated: pins and needles, numbness, altered reflexes, or weakness (needs timely assessment)
- Difficulty with usual activities such as sitting tolerance, bending to dress, lifting, sport, or prolonged walking
Aggravating Factors
- Prolonged sitting, especially in a slumped posture, or long periods of driving without breaks
- Repeated forward bending (flexion), particularly combined with twisting or lifting
- Heavy lifting, especially if it is sudden, fatigued, or outside your usual training or work tolerance
- High-volume work or sport with repeated spinal loading (manual handling, gym training spikes, running load spikes)
- Sustained postures (standing, sitting, or bent positions) with minimal movement variation
Causes
Discogenic low back pain is usually linked to a combination of disc tissue sensitivity and load management. It occurs when the intervertebral disc becomes sensitive and less tolerant to load, meaning symptoms can flare when the demands placed on the disc exceed what it can currently manage — either suddenly or gradually. This may happen after a sudden overload (such as a heavy lift, a long day of bending, or a sharp increase in training), or through repeated micro-loading over time (such as prolonged sitting with limited movement breaks, repetitive bending for work, or building lifting volume faster than your capacity). When the disc is overloaded, the outer layer (the annulus) can become sensitised, and inflammatory chemicals may amplify pain signals in nearby tissues. In some cases, disc material and inflammation can also irritate the adjacent nerve root, which is when leg symptoms may occur. Even then, symptoms often improve with conservative care, appropriate pacing, and progressive rehabilitation.
Terminology you might see on scans or in reports (terms are related but not identical):
- Disc degeneration: age-related changes in disc hydration and structure, commonly seen on imaging and often not painful on its own.
- Disc strain / disc overload: a flare of disc sensitivity related to a recent increase in pressure or load, often linked with bending, lifting, or prolonged flexion.
- Disc bulge: the outer margin of the disc extends beyond the normal edges over a broad base.
- Disc herniation: a localised displacement of disc material beyond the normal disc margin (includes protrusion and extrusion).
These definitions are described in lumbar disc nomenclature resources used internationally for consistent reporting. In practice, physiotherapy management is guided more by your symptoms, function, and neurological findings than by terminology alone, unless an injection or surgery is being considered.
How Is It Diagnosed?
Discogenic low back pain is primarily diagnosed clinically by a physiotherapist or doctor. Your clinician will ask about how symptoms started, what makes them better or worse, and whether there are any warning signs that suggest a more serious condition. The assessment focuses on your movement profile, functional limitations, and whether nerve irritation is present. A physiotherapy examination commonly includes observing how you move (bending, returning upright, walking, changing positions), checking which movements reproduce symptoms, and assessing strength and control of the trunk and hips. If leg symptoms are present, your physio will test neurological function including sensation, reflexes, and muscle strength (myotomes), and will screen for red flags such as progressive weakness or bowel and bladder changes.
Physiotherapists also consider other sources of low back pain. Facet joints, sacroiliac joints, hip issues, and sensitised muscles can mimic disc symptoms. This is why a hands-on assessment is important, and why a scan is not always necessary to create an effective rehab plan.
Imaging is generally reserved for suspected serious pathology, severe or progressive neurological symptoms, or when results would change management (e.g., planning an injection or surgery). Routine imaging is rarely helpful in uncomplicated low back pain and may lead to incidental findings.
Investigations & Imaging
- MRI
- Shows disc hydration, bulge/herniation, annular changes, and potential nerve root contact. Useful when severe or progressive neurological symptoms are present, or when results would change management (such as injection or surgical planning).
- X-ray
- Does not visualise discs well, but may be used to check alignment or other bony causes when clinically indicated.
- CT scan
- May be used when MRI is not possible, or for specific bony detail, but is not first-line for most discogenic presentations.
- Neurological examination (clinical test)
- Strength, reflexes, and sensation testing helps identify nerve root involvement and guides urgency of referral and treatment focus.
Grading / Classification
- Disc degeneration
- Age-related changes in disc structure and hydration. Common on imaging and may or may not be related to symptoms.
- Disc bulge
- Broad-based extension of the disc margin beyond the normal disc space boundaries.
- Disc herniation
- Localised displacement of disc material beyond the normal margin, including protrusion and extrusion, using standard nomenclature definitions.
- Radiculopathy
- Nerve root involvement causing neurological signs such as altered sensation, reflex changes, or weakness in a myotomal pattern. This changes management priorities and may warrant imaging if severe or worsening.
Physiotherapy Management
Discogenic low back pain is commonly managed in physiotherapy using a simple principle: settle symptoms first, then rebuild capacity. Most people do not need their back “fixed” or “put back in”. Instead, the goal is to calm the sensitised disc and surrounding tissues, restore normal movement patterns, and progressively increase what your spine can tolerate.
Many disc-related episodes improve significantly over time with good advice, staying active within tolerable limits, and graded rehabilitation. Physiotherapy is especially valuable when pain is limiting function, when symptoms keep flaring with daily life, or when leg symptoms are present and need close monitoring.
Exercise
Physiotherapy exercises are selected based on how your symptoms respond and which movements ease or aggravate them. Early on, the goal is often to find a “direction of comfort” that reduces symptoms and helps you feel more confident moving again. For some people this involves extension-based exercises (gentle arching movements), particularly when forward bending and sitting are strong triggers. For others, it may focus on neutral-spine control, hip-dominant movement retraining, or a gradual return to bending if movement has become limited or uncomfortable over time.
As pain becomes more manageable, rehab focuses on building strength and endurance of the trunk, hips and legs so the spine is not repeatedly overloaded by everyday tasks. This commonly includes progressive walking, loaded carries, hip hinging strength, glute strength, and trunk endurance work. For people returning to gym training, physiotherapy often includes graded exposure to squats, deadlifts, and bending patterns with technique modifications that keep symptoms stable while capacity improves.
If you have leg symptoms, your physiotherapist will also include exercises that aim to reduce nerve sensitivity (when appropriate), while still improving spinal load tolerance. Exercise selection is not one-size-fits-all. It is guided by your response during the session and in the 24 to 48 hours after.
Activity Modification
Early load management is often the biggest lever for discogenic pain. That usually means temporarily reducing the specific loads that spike symptoms, without stopping all movement. Common examples include limiting prolonged sitting, breaking up driving with short walks, avoiding repeated end-range bending, and modifying heavy lifting while the disc is irritable.
Physiotherapists often use a pacing approach: you keep moving, but you dose your activities so the disc settles rather than being repeatedly stirred up. This might include shorter sitting blocks, frequent posture variation, and swapping high-irritation tasks for alternatives while you continue rehab. As your symptoms improve, activity modification shifts to a planned return to bending and lifting so you do not become restricted or fearful. This is where physiotherapy guidance can prevent the cycle of flare-ups.
Manual Therapy
Hands-on treatment can be useful in the early stages to make movement easier and reduce pain, even though it does not “realign” the spine or push a disc back in. Physiotherapists may use joint mobilisation, mobilisation with movement, and soft tissue techniques to reduce protective muscle guarding and improve comfort so you can move and exercise more normally.
It’s often the case that joints around the affected area are restricted. Mobilisation techniques in these regions can be extremely helpful in regaining overall mobility and reducing strain through the disc.
Manual therapy is generally used to support active rehab. The aim is to reduce sensitivity, improve motion tolerance, and help you re-engage with walking and strengthening. Your physiotherapist will choose techniques based on your presentation, irritability, and preferences.
Bracing & Taping
Taping or a temporary lumbar support (such as a support pillow or towel roll) may help some people with discogenic low back pain, particularly during sitting or driving, by reducing sustained end-range postures and improving comfort. These supports are usually short-term tools rather than long-term solutions.
A physiotherapist can show you how to use support strategically, for example during long car trips or early return-to-work days, while you continue building strength and tolerance through exercises. The goal is to rely more on improved capacity and movement confidence over time, not on external support permanently.
Dry Needling
Dry needling may be used when muscle spasm and protective tightness are significant contributors to your symptoms. In discogenic low back pain, muscles in the lumbar region, glutes, and hips often tighten as a protective response. If dry needling is appropriate for you, the aim is to reduce muscle guarding so you can move more freely and participate better in walking and strengthening.
Dry needling is optional and not required for everyone. It is generally most helpful when combined with a clear activity plan and progressive exercise program.
Heat & Ice
Heat can be a simple and effective comfort strategy for discogenic low back pain, particularly when muscle guarding is prominent or when symptoms are worse after sitting. A heat pack may help you move more comfortably and can be used before gentle mobility or walking. Ice is less commonly used for discogenic pain, but some people prefer it in the very early, sharp phase. Your physiotherapist can guide what suits your symptom pattern and how to use these tools to support activity rather than replace it.
Education
Education is one of the most valuable parts of physiotherapy for disc-related low back pain. Your physiotherapist will help you understand common disc terms, why scan findings don’t always match pain, and why your spine is strong rather than fragile. Education also includes practical advice on sitting, lifting, and moving in ways that keep symptoms manageable while your capacity rebuilds.
Your physiotherapist will also explain when imaging is actually helpful. In most cases of uncomplicated low back pain, early imaging isn’t recommended because it rarely changes treatment and can uncover incidental findings that lead to unnecessary worry or interventions. This helps you make informed decisions about next steps if symptoms persist.
Other
Other physiotherapy strategies can include graded return-to-work planning, gym technique coaching, and building a long-term conditioning program. If symptoms are not improving over time, your physiotherapist may recommend medical review to discuss whether imaging, injections, or specialist input would genuinely change management. In many cases, a solid trial of physiotherapist-led rehabilitation is recommended before considering invasive options, provided symptoms are stable and there are no red flags.
Other Treatments
Other treatments may include short-term pain relief (for example paracetamol or anti-inflammatory medication when appropriate) guided by a pharmacist or GP. In selected cases, a GP or specialist may discuss image-guided injections, particularly when nerve root irritation is a major driver of symptoms and conservative care has not provided enough relief.
These options are generally most effective when paired with a structured physiotherapy program, because medication or injections do not rebuild strength, movement confidence, or load tolerance on their own.
Surgery
Surgery is not required for most cases of discogenic low back pain. Surgical discussion is more relevant when there is significant or progressive neurological deficit, severe persistent leg symptoms consistent with nerve root compression, or when conservative care has not provided an acceptable outcome and imaging findings match the clinical picture.
If surgery is considered, physiotherapy remains important both before and after. Pre-surgical physiotherapy helps maintain strength and function, while post-surgical rehabilitation focuses on restoring mobility, rebuilding strength, and returning to work and sport safely.
Prognosis & Return to Activity
The outlook for discogenic low back pain is often favourable. Many people improve over the first few weeks with good advice, staying active within tolerable limits, and a progressive strengthening plan. Even when a disc bulge or herniation is present, symptoms can settle over time, and disc material can reduce in size in many cases.
Return to activity is guided by function and symptom behaviour rather than a scan finding. Physiotherapists often use a “24-hour response” rule: if you can do an activity with manageable symptoms during the task and no significant flare-up the next day, it is usually a safe step. If symptoms ramp up strongly for 24 to 48 hours, the load likely needs to be adjusted. With this approach, most people can steadily expand what they can do and return to normal work, sport, and exercise.
Complications
- Persistent or recurrent flare-ups if bending and lifting loads are reintroduced too quickly without rebuilding capacity.
- Ongoing leg symptoms or neurological deficit if nerve root irritation is significant and not monitored appropriately.
- Fear-avoidance and deconditioning if activity is stopped completely for long periods, leading to reduced tolerance and confidence.
Preventing Recurrence
- Build a resilient back with ongoing strength and endurance training for the trunk and hips, not just stretching. This reduces future disc overload with work and sport.
- Avoid sudden spikes in lifting, bending, or training volume. Progress loads gradually so your disc capacity keeps pace with demand.
- For desk work and driving, vary posture and take regular movement breaks to reduce prolonged flexion loading through the lumbar discs.
- Practise efficient lifting habits (hip hinge, keep loads close, avoid rushed twisting under load), especially when tired or under time pressure.
When to See a Physio
- If low back pain is limiting work, sleep, sitting tolerance, or daily tasks for more than 1 to 2 weeks.
- If pain keeps flaring every time you try to return to bending, lifting, gym training, or sport, and you need a graded plan.
- If you have leg pain, pins and needles, numbness, or weakness and want assessment of nerve involvement and safe progression.
- Seek urgent medical care if there is progressive weakness, saddle numbness, or changes to bowel or bladder control.