A pars interarticularis defect injury, commonly referred to as a pars defect, is a condition that affects a small but important segment of bone in the spine. It is most frequently seen in children and adolescents who participate in sports that involve repetitive bending backwards or twisting movements of the lower back. Activities such as gymnastics, ballet, and cricket, particularly fast bowling, place high repetitive loads on this area of the spine.
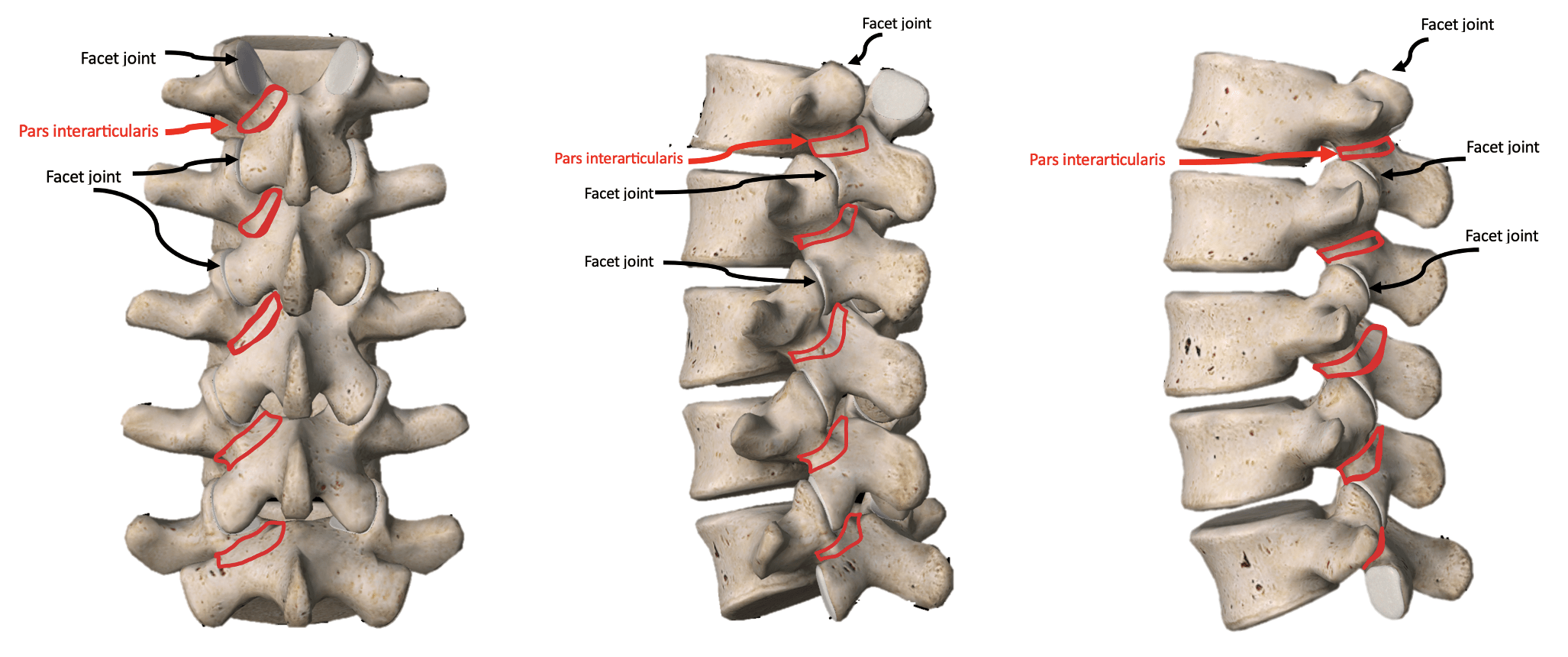
The pars interarticularis is the bony bridge that connects the upper and lower facet joints of a vertebra. Injury to this structure can occur on one side of the spine (unilateral) or both sides (bilateral). Early recognition and appropriate physiotherapy management are critical to reduce the risk of progression and support a safe return to sport.
Key Facts
- Pars interarticularis injuries are most commonly diagnosed in adolescents involved in extension-based sports such as gymnastics and cricket.
- Early diagnosis and physiotherapy management significantly improve recovery time and reduce the risk of progression to fracture.
Risk Factors
- Adolescent growth spurts
- High training loads or rapid increases in training volume
- Sports requiring repetitive lumbar extension and rotation
Symptoms
- Localised lower back pain that worsens with extension or rotation
- Pain during sport, particularly activities involving back bending
- Stiffness or reduced movement in the lower back
- In more advanced cases, leg pain or neurological symptoms
Aggravating Factors
- Repetitive lumbar spine extension
- High training volumes without adequate rest
- Fast bowling, tumbling, back walkovers, or arabesque positions
Causes
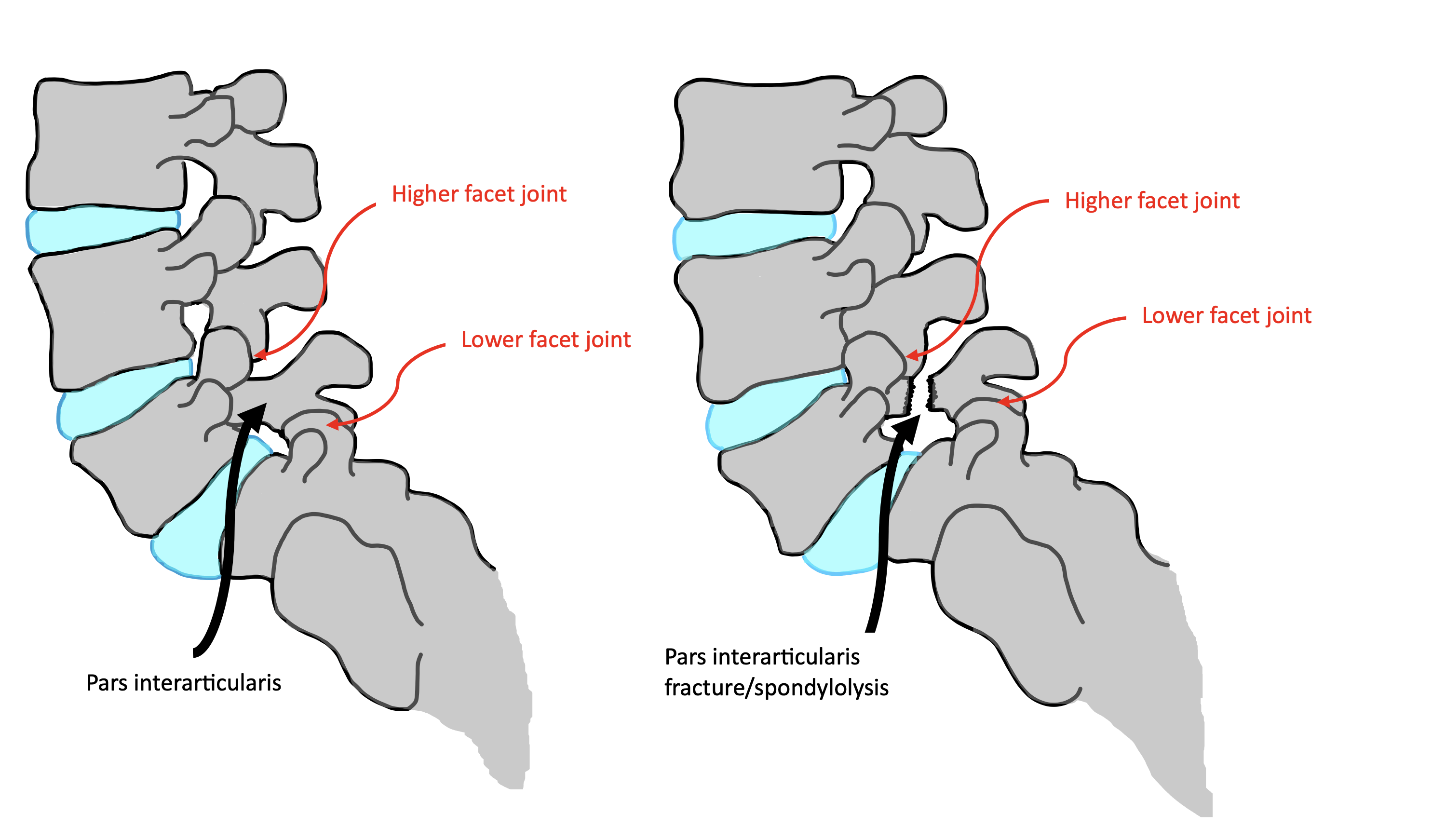
A pars interarticularis defect injury is most commonly caused by repetitive overuse rather than a single traumatic event. Repeated lumbar hyperextension and rotational forces place stress through the pars interarticularis. When these loads exceed the bone’s capacity to adapt and recover, a stress response can develop.
If the stress continues without adequate rest and load modification, the bone stress may progress to a stress fracture, also known as a spondylolysis. This progression highlights the importance of early physiotherapy assessment and appropriate training modification in young athletes.
How Is It Diagnosed?
Diagnosis of a pars interarticularis defect injury begins with a thorough history and physical assessment by a healthcare professional, often a physiotherapist or sports medicine specialist. The assessment focuses on pain behaviour, aggravating movements, spinal mobility, and functional capacity.
Clinical findings guide whether imaging is required. Imaging is used to confirm the diagnosis and determine the severity of the injury, which is essential for guiding management and return-to-sport decisions.
Investigations & Imaging
- MRI scan
- Most sensitive imaging to identify early bone stress, oedema, or stress reactions in the pars interarticularis
- CT scan
- Used to determine whether a complete pars fracture is present and assess bony integrity
- X-ray
- May identify chronic pars fractures or vertebral slippage but cannot detect early bone stress
Grading / Classification
- Bone stress reaction
- Early stage injury with bony oedema and no fracture, highly responsive to load modification and physiotherapy
- Unilateral pars fracture
- Complete fracture on one side of the vertebra with longer recovery but good return-to-sport potential
- Bilateral pars fracture
- Fracture on both sides, increasing the risk of instability and spondylolisthesis
Physiotherapy Management
Physiotherapy management of a pars interarticularis defect injury focuses on reducing load through the injured bone, supporting healing where possible, and restoring strength and control to the trunk and hips. Management is closely guided by injury severity and imaging findings.
Exercise
Exercise rehabilitation is a core component of physiotherapy for pars injuries. Early programs emphasise pain-free core stability, trunk control, and hip strength while avoiding excessive lumbar extension. Exercises are progressed gradually from static control to dynamic movements as symptoms allow.
Activity Modification
Activity modification is essential to allow the pars to recover. This includes temporary restriction of aggravating activities such as back bending and rotation, with a graded return to sport under physiotherapy guidance.
Manual Therapy
Manual therapy may be used by physiotherapists to address secondary stiffness or muscle tightness in surrounding regions, supporting improved movement without placing stress on the injured pars.
Heat & Ice
Heat or ice may be used for symptom relief, particularly to manage associated muscle discomfort during rehabilitation.
Education
Education is vital in pars injury management. Physiotherapists provide clear guidance on healing timelines, safe movement, and the importance of load management to reduce fear and support adherence.
Other
Rehabilitation is often coordinated with sports medicine specialists and other healthcare providers to address nutrition, training load, and overall health factors influencing bone recovery.
Other Treatments
In some cases, bracing or medical management may be used alongside physiotherapy, particularly in early stress injuries or when symptoms are difficult to control.
Surgery
Surgery is reserved for severe cases such as bilateral pars fractures with instability, spondylolisthesis, or neurological symptoms. Surgical decisions are made by a specialist and followed by structured rehabilitation.
Prognosis & Return to Activity
Prognosis depends on injury severity. Early-stage pars stress injuries often recover fully within 3 to 6 months. Unilateral fractures require longer rehabilitation, while bilateral fractures may need specialist intervention.
Complications
- Progression to spondylolisthesis
- Chronic low back pain if not appropriately managed
- Nerve root irritation or compression
Preventing Recurrence
- Manage training loads and avoid excessive lumbar extension during growth periods
- Maintain trunk and hip strength to reduce stress on the pars interarticularis
- Seek early physiotherapy assessment for persistent back pain in young athletes
When to See a Physio
- Persistent back pain in a young athlete
- Pain worsening with extension-based activities
- Back pain associated with leg symptoms or reduced performance