Rotator Cuff Related Shoulder Pain (RCRSP) is one of the most common causes of shoulder pain. It is an umbrella term that includes conditions such as sub-acromial shoulder pain, sub-acromial bursitis, rotator cuff tendinopathy and rotator cuff tendinitis.
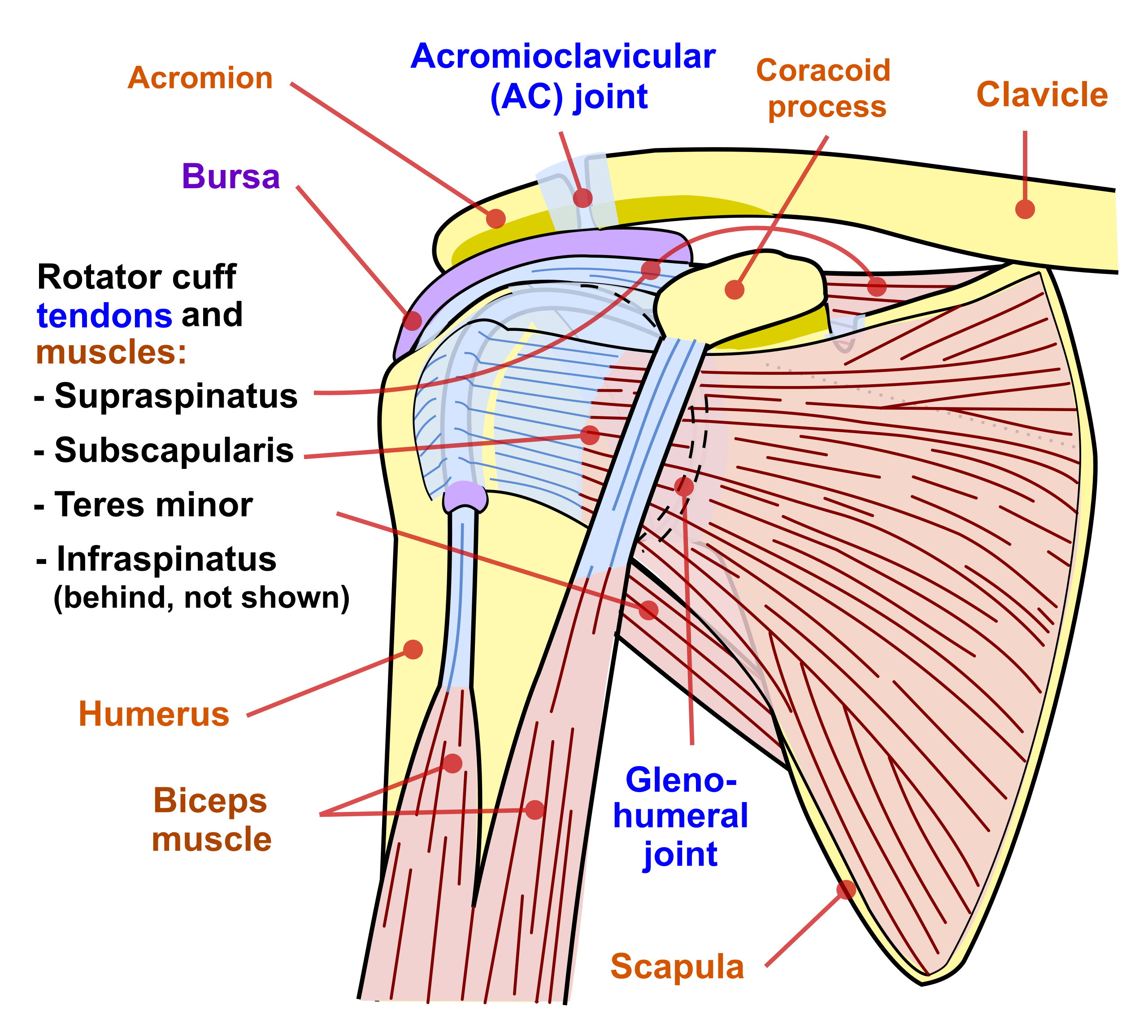
The rotator cuff is a group of four muscles and their tendons that help stabilise the shoulder and control movement. These tendons, along with the sub-acromial bursa (a fluid-filled sac that reduces friction), sit underneath the acromion bone at the top of the shoulder. When these structures become irritated or overloaded, pain develops.
RCRSP usually develops gradually and is rarely caused by a single traumatic incident. It often occurs after a change in shoulder loading, such as performing new overhead tasks, lifting heavier weights, or doing repetitive movements.
Physiotherapy for rotator cuff related shoulder pain is the mainstay of treatment. A physiotherapist can assess your shoulder function, identify contributing factors such as weakness or altered movement, and provide a tailored rehabilitation plan to reduce pain and restore strength.
Key Facts
Risk Factors
- Age over 40
- Poor rotator cuff and scapular muscle strength
- Previous episodes of shoulder pain
- Poor posture (rounded shoulders, forward head position)
- High or sudden increases in shoulder load (e.g. starting a new sport or job)
- Smoking, poor sleep, or general health issues that reduce tissue healing capacity
Symptoms
- Pain on the outside or front of the shoulder
- Pain when lifting the arm overhead
- Night pain, particularly when lying on the affected side
- Weakness with lifting or rotating the arm
- A catching or pinching sensation in the shoulder
- Reduced ability to perform daily activities such as hanging washing, lifting groceries, or reaching into cupboards
Aggravating Factors
- Repetitive overhead movements (e.g. shoulder press at the gym)
- Sustained overhead positions (e.g. painting a ceiling, hanging washing)
- Lifting heavy objects away from the body
- Using vibrating tools
- Sudden increase in gym training load, especially pressing exercises like bench press
- Sleeping with the arm overhead or lying on the painful side
Causes
Rotator cuff related shoulder pain is generally caused by a mismatch between the load placed on the shoulder and the capacity of the rotator cuff and surrounding tissues to handle that load.
- Load includes all activities performed with the shoulder such as exercise, lifting, carrying, sports, and repetitive work.
- Capacity refers to how much load the tissues can tolerate, which is influenced by factors such as muscle strength, tendon health, age, general fitness, sleep, and stress.
When load exceeds capacity, the rotator cuff tendons and bursa may become irritated, leading to pain. Unlike traumatic shoulder injuries (e.g. dislocations), RCRSP usually develops gradually, especially after sudden changes in training or daily activities.
How Is It Diagnosed?
A physiotherapist can usually diagnose RCRSP through a detailed history and physical examination. Key aspects include:
- Identifying activities that aggravate symptoms
- Assessing strength of the rotator cuff and scapular muscles
- Testing shoulder range of motion
- Checking for postural or movement deficits
Unlike some shoulder conditions, imaging is not always required, as clinical assessment is often sufficient to guide treatment.
Investigations & Imaging
- Ultrasound
- Can detect bursitis, tendon thickening, or tears.
- MRI
- Provides detailed imaging of rotator cuff tendons and is useful if a large tear is suspected.
- X-ray
- May be used to rule out arthritis or bony changes that could reduce sub-acromial space.
Physiotherapy Management
Exercise
Exercise is the foundation of physiotherapy for rotator cuff related shoulder pain. Early in rehabilitation, your physiotherapist may prescribe isometric exercises, which involve contracting the shoulder muscles without moving the joint. These help reduce pain while maintaining muscle activity. As symptoms improve, the program progresses to strengthening exercises targeting the rotator cuff muscles, the scapular stabilisers, and the postural support muscles of the upper back. Eventually, functional movements such as lifting and reaching are introduced to ensure your shoulder can tolerate everyday demands, work tasks, and sporting activities. Exercises may include resistance band external rotations, scapular retraction drills, and controlled overhead strengthening.
A structured home exercise program is essential for long-term success. Physiotherapists monitor and progress exercises at regular reviews to ensure steady improvement while avoiding flare-ups. In many cases, physiotherapy alone is enough to restore full function and prevent recurrence.
Activity Modification
Rather than stopping all activity, physiotherapy focuses on modifying how you use your shoulder to reduce irritation. This might mean reducing repetitive overhead tasks, limiting pressing exercises at the gym, or adjusting your workstation setup to minimise overhead reaching. By making these short-term changes, your shoulder is allowed to settle while still keeping you active and maintaining general fitness.
Manual Therapy
Manual therapy techniques such as soft tissue release and joint mobilisation may be used in the short term to relieve pain and improve mobility. Soft tissue treatment around the shoulder and upper back can reduce muscle tension, while mobilisation of the shoulder joint can help restore range of motion if stiffness has developed. These approaches are always used alongside exercise, rather than as stand-alone treatments.
Postural Retraining
Many people with rotator cuff related shoulder pain present with rounded shoulders or altered movement of the shoulder blade. This can increase compressive load on the rotator cuff tendons and bursa. Postural retraining forms an important part of physiotherapy, using a combination of education, stretching, and strengthening exercises to restore better shoulder blade control and positioning. This helps reduce pain and improves efficiency of movement during daily tasks and sport.
Bracing & Taping
Taping techniques may be used during rehabilitation to offload painful structures and provide short-term pain relief. Kinesiology tape or rigid taping can help reduce strain on the rotator cuff tendons, making it easier to continue with activity and exercise. While taping is not a long-term solution, it can be particularly useful during sport, work, or heavier activities while you build strength through rehabilitation.
Dry Needling
Dry needling may be offered to release tension in overactive muscles around the shoulder and upper back. This can provide short-term relief and help improve comfort during exercise. However, it is always considered an adjunct treatment and should be combined with a structured strengthening program for best results.
Shockwave
Shockwave therapy is sometimes considered for persistent rotator cuff related shoulder pain that has not improved with exercise and manual therapy. Evidence for its effectiveness is mixed, but in some cases it may help stimulate tendon healing and reduce pain, particularly when there are chronic changes in the tendon.
Heat & Ice
Both heat and ice can be used to help manage symptoms. Ice is often recommended in the early stages or after flare-ups to reduce irritation and numb pain. Heat may be more useful in longer-standing cases where stiffness is present, as it helps improve circulation and relax tight muscles around the shoulder.
Education
Education is one of the most important components of physiotherapy for rotator cuff related shoulder pain. Understanding the concept of “load versus capacity” helps patients recognise why their shoulder became painful and how to manage it effectively. Physiotherapists provide clear guidance on what movements are safe, what activities should be modified, and how long recovery is likely to take. Most people are advised to allow at least 12 weeks of structured rehabilitation before considering other treatment options.
Other Treatments
Corticosteroid injections may provide short-term pain relief but do not address the underlying problem. They may be considered if pain is limiting rehabilitation progress.
Surgery
Surgery is rarely the first option for rotator cuff related shoulder pain. Procedures such as sub-acromial decompression have not been shown to provide significant benefit over physiotherapy. Surgery may only be considered if:
- Symptoms persist beyond 6–12 months despite physiotherapy
- There is a confirmed large or full-thickness rotator cuff tear causing significant weakness
Prognosis & Return to Activity
Most people with rotator cuff related shoulder pain improve significantly with physiotherapy. The majority will recover within 12 weeks, though some may require longer rehabilitation.
Return to sport or work depends on:
- The severity and duration of symptoms
- Adherence to exercise rehabilitation
- Individual factors such as age and overall health
With physiotherapy, the majority of patients can return to full activity without surgery.
Complications
- Persistent pain if untreated
- Loss of shoulder strength and function
- Tendon degeneration or tearing over time
- Reduced ability to participate in sport or overhead activities
Preventing Recurrence
- Avoid sudden increases in overhead training loads
- Maintain regular shoulder and upper back strengthening exercises
- Optimise workplace ergonomics to limit reaching
- Address posture to reduce compressive load on the rotator cuff and bursa
- Build training gradually after breaks to avoid overload
When to See a Physio
- Shoulder pain lasting more than 1–2 weeks
- Pain interfering with sleep
- Difficulty lifting or reaching overhead
- Weakness or loss of shoulder function
- Recurring shoulder pain after activity