Bone Stress Injuries (BSI) or Stress Fractures in an athletic population exist on a spectrum of disrepair which will progress in an environment where the tissue is being inappropriately loaded. It is for this reason that Stress Fractures are largely preventable and should not be missed when presenting in the early stages.
Understanding Bone Stress
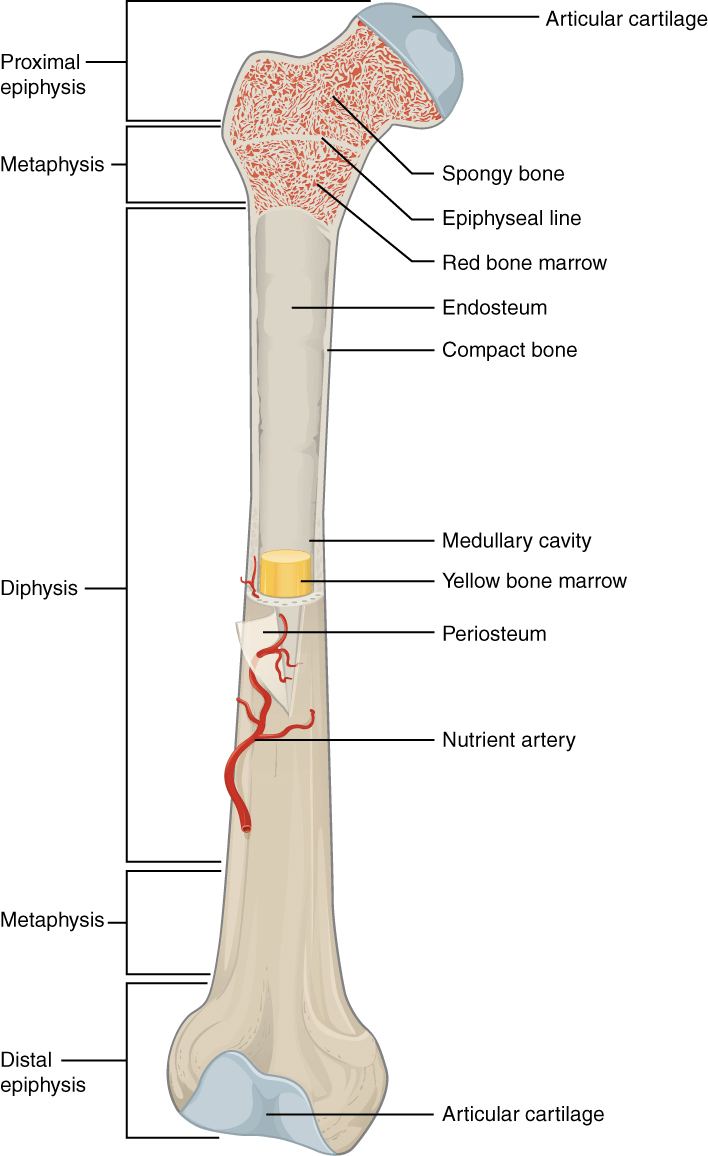
The makeup and structure of bone is layered to provide support and strength to withstand torsion or force. Long bones are separated into sections called the Diaphysis and Epiphysis, both are separated by a Metaphysis. The Diaphysis is comprised of a marrow filled cavity and surrounded by Cortex and Cortical bone. The Cortex connects to the Periosteum and subsequently Spongy Bone. Lining the medullary cavity is the Endosteum which is where we will shift our attention to briefly.
Bone Resorption and Formation
Within the Endosteum and Periosteum there are a unique group of 4 cells; Osteogenic, Osteoclasts, Osteoblasts and Osteocytes. The Osteoclasts facilitate resorption of the bone and the Osteoblasts allow for bone formation, typically sitting in areas of growing bone. The initial response to loading is breaking down of bone, followed by resorption and formation of new bone. However, new bone formation is a slower process than bone resorption.
Typically, it takes 1-2 weeks for the process of bone resorption and formation to take place. Therefore, if bones are loaded too much in this period, resorption occurs too quickly for new bone formation to keep up. This can lead to gradual weakening of the bone and eventual stress fractures if continued.
Bone Stress Injuries vs. Stress Fractures
Bone stress injuries exist on a continuum of severity. Early on, stress injuries are referred to as “stress reactions”, meaning the bone is trying reacting to the increase in load. In this stage, the bone begins to weaken as resorption occurs faster than bone formation. If excessive loading of the bone continues and training is not adjusted, these injuries progress further along the continuum as the bone becomes weaker and weaker. Eventually, we begin to see cracks forming in affected areas, which lead to a stress fracture.
It is important to address bone stress injuries early on. The further along the continuum of severity, the longer the recovery process will be.

Risk Factors
Increases in training load without proper recovery time to allow bones to adapt to a new load are the primary cause of bone stress injuries. However, there are some other factors that can increase the risk of developing a bone stress injury. These include:
- Diet: Insufficient calorie intake relative to amount of exercise performed.
- Vitamin D deficiency.
- Female Athlete Triad:
- Eating disorders.
- Abnormalities in menstrual cycles, primarily Amenorrhea or Oligomenorrhea.
- Decreased bone density.
Signs and Symptoms
- Gradual onset of pain with no obvious mechanism of injury or moment in time pain began.
- Recent increase in activity levels or extended periods of high activity.
- Tenderness to touch over the injured area.
- Pain can be present at rest, or at night-time.
Imaging
If a bone stress injury is suspected, imaging to confirm diagnosis is often indicated. An X-ray may show evidence of a bone stress injury, however they often appear normal and are not sensitive enough to detect injuries in the early stages. Repeat X-rays can be done if pain persists to identify any progression of injury.
CT scans are slightly more sensitive than X-ray, and are helpful to rule out other diagnoses.
Overall, MRI is the gold-standard imaging option. MRI has an 88% sensitivity when diagnosing bone stress injuries, and will also show any soft tissue damage (muscles, ligaments, tendons etc). This makes MRI’s not only useful for confirming bone stress injuries, but also ruling in and out other structures being involved in symptoms.
Due to X-rays being cost-effective, and easily accessible, this might be an appropriate initial imaging option. However if symptoms are not improving, and pathologies not appearing on X-ray, an MRI should be conducted.
Treatment
Management of bone stress injuries vary depending on the severity. Treatment of low-risk stress injuries involves:
- Ceasing aggravating activities for a short period.
- Weight bearing as tolerated. If walking is painful, crutches may be necessary.
- Pain relief medication as needed.
- Once pain is reduced, a gradual return to activity should begin. It is important to start with a low load, and very gradually build back up to previous levels of activity.
- During this time, strengthening exercises should be completed to; reduce loss of strength when not completing normal activities, and to address any deficiencies that may have lead to injury in the first place.
If imaging showcases a more severe injury, at a high-risk site such as the tibia or femur, referral to an orthopaedic specialist may be indicated to discuss further options for management.
References:
Kiel J, Kaiser K. Stress Reaction and Fractures. [Updated 2023 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507835/