Overview
Tendinopathies fall under the umbrella term of overuse injuries, and are one of the most commonly seen musculoskeletal injuries. They can occur in any tendon throughout the body, and are mostly caused by a sharp increase in load/activity, but can also develop from extensive use over a long period of time.
Some of the most common sites for tendinopathies to occur are in the Achilles, Patella, Gluteal, Biceps or Rotator Cuff tendons.
What is a Tendon?
Tendons are strong, connective tissue that join muscle to bone. They are involved in moving the body as muscles contract, and they absorb a lot of force. Tendons are built to be tight and stiff, like a rope, as this allows them to best absorb the forces created in activities like walking and jumping. Although tendons do not contract, they do have elastic properties. This allows them to generate movement by acting like a spring.
So not only do tendons absorb a lot of energy, they also store and release it. This means tendons go through a lot during high speed and impact activities, such as running and jumping, as well as sports like basketball.

What is a Tendinopathy?
Normally, healthy tendons are stiff, this makes them suitable for quick storage and release of load. When we change our activity levels, such as beginning a new sport, our body has to adapt to this new load. Tendon’s adapt to increased work by becoming more stiff, this makes them stronger and allows them to act more efficiently.
Tendons are made up of what are called collagen fibres. In healthy tendons, these fibres are aligned nicely and neatly in a parallel fashion.
When the activity load (duration, intensity or type) increases before the tendon can adapt to the demand, the “overloaded” structure attempts to rush to get stronger. The collagen fibres become unaligned, resulting in a thicker, less stable and overall weaker tendon. This is how a tendinopathy begins.
Previously these injuries were referred to as Tendonitis (‘itis’ meaning inflammatory). This is because it was thought that inflammation was a primary factor in these injuries, however this is now known to not be the case. Although inflammation is still involved to some extent, there are a multitude of complex physiological changes that occur in tendinopathies.
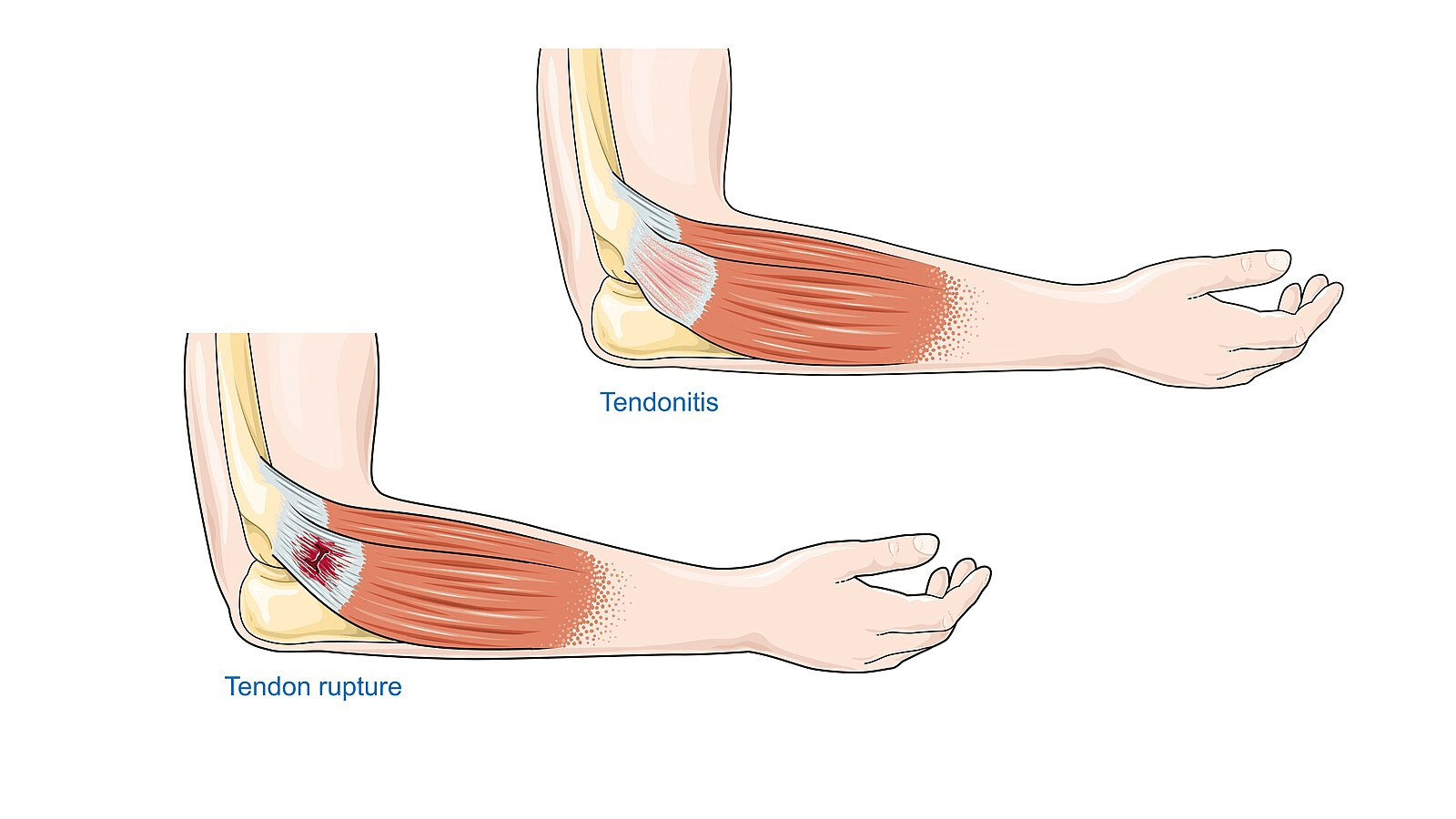
.jpg){kind=link}
Stages of Tendinopathy: A Continuum
Pain and function in tendinopathy can come and go in waves. It’s common that some cases of tendinopathy respond well to treatment and recover quickly, whereas some cases can be more resistant and take a lot longer.
An explanation of this is a model that proposes Tendinopathy to be a continuum. There are three stages of tendinopathy, in which the affected tendon moves in and out of. Movements along this continuum, are mostly driven by changes in load. Tendons may also be within two stages at the one time.
Stage 1: Reactive
This is the tissue’s response to acute overload. The cells within the tissue become more proliferative, meaning they rapidly grow in size and number. This leads to short-term tendon thickening.
This adaptation reduces short-term stress on the tendon, and will not result in any immediate changes within the collagen fibre alignment. With load reduction and treatment, the tendon will likely return to normal reasonably quickly. However if overloading continues, the tendon can progress to the next stage.
Although the reactive stage is the earliest, it is typically the most painful.
Stage 2: Dysrepair
The response within cells are similar to the reactive stage, but on a larger scale. Protein production will begin to increase, resulting in disorganisation of collagen fibres.
Weakness begins to develop in the tendon, and we may also see an increase in inflammation and vascularisation (blood flow).
Load management and treatment can help this tendon return to normal, but the process will be longer.
Stage 3: Degenerative
This is the most advanced stage of tendinopathy. The above changes have continued and progressed to result in cell death and trauma within the tendon. This means affected areas are disorganised, and filled with blood vessels now rather than the tightly knit collagen fibres seen in healthy tendons.
Capacity for affected areas to recover in this stage is low, however the entire tendon is not degenerative, and thus rehabilitation involves the still relatively healthy sections.

Pain in Tendinopathy:
Pain experienced in tendinopathy is not always directly related to the structural changes displayed above. Although degenerative tendons are the most structurally affected, they are often not as painful as reactive tendons. This is likely because there is poor sensory innervation in deep tendon tissue, where most structural changes occur.
Pain in tendinopathy is typically seen in two cases:
- Pain during an acute overload as a reactive tendinopathy.
- Pain when healthy parts of a degenerative tendon become reactive.
Tendons can be within two of the above stages at the same time. This is referred to as a Reactive on Degenerative Tendinopathy. Degenerative portions of a tendon are not as functional or strong, meaning healthy parts are required to work harder. This means the healthy parts of the tendon are now more susceptible to overload, and thus becoming reactive.
The Role of the Nervous System
There is some evidence that the nervous system has a role in tendinopathy pain and function. This theory is very complex, and this article will only provide a brief summary.
It has been demonstrated that people with tendinopathy have altered cortical inhibition, and corticospinal excitability compared to those without tendinopathy. This means the brain could have a different response (pain) to stimulus (load) in the tissue. This in turn alters the way muscles surrounding the tendon activate.
Those with tendinopathy have been shown to have decreased muscle activation surrounding the tendon, this is thought to be a protective mechanism as an attempt to offload the tendon. Although this can be helpful, it also alters biomechanics in running and jumping, which may in turn lead to more tendon loading.
Interestingly, differences in cortical inhibition and excitability are demonstrated on the unaffected side as well. This can lead to an increased risk of developing a reactive tendinopathy on the unaffected side. It also means that rehabilitation focusing on the unaffected side can impact loading patterns and neural activity, potentially benefitting the affected side.
Addressing the involvement of the nervous system in tendinopathy is often a missed part of rehab. Normal programs may return the tendon to normal, however the changes in neural activity and surrounding muscle behaviour often remain, resulting in high rates of injury recurrence.
Signs and Symptoms of Tendinopathy
Some signs that you might have a tendinopathy include, but are not limited to:
- Pain related to excessive use over a long period of time, or pain associated with an increase in load/change in activity.
- Gradual onset of pain, without any clear mechanism of injury.
- Pain at the beginning, during or after activity.
- Pain decreasing throughout activity, as tendons warm up.
How are they Treated?
Load Management:
The first-line of treatment in tendinopathy is load management. This means we stop doing the aggravating tasks as much as we can for a short period. This allows the tendon time to recover. During this time, your therapist may show you some isometric exercises. Isometric means the muscle is contracting, but not moving. These types of exercises are low load, and have been shown to have pain relieving benefits.
Strengthening:
Once pain is reduced, the tendon needs to be reloaded to increase it’s capacity. This is completed gradually through a combination of individualised isometric, heavy slow concentric, and eccentric exercises. These types of exercises help to realign the collagen fibres of the tendon.
As tendon capacity increases and pain levels reduce, plyometrics can be introduced if tolerable. As we know, tendons take the most load during high speed and impact activities like jumping and running. To ensure the tendon can cope with the load it experiences during normal activity, we need to expose it to faster movements than it experiences during isometric, heavy slow resistance and eccentric exercises. This helps to restore the tendons elastic properties. This should be done progressively, through exercises like ankle pulsing, then hopping and finally jumping activities.
Strengthening is reasonably similar regardless of whether a tendon is considered reactive or degenerative. Although we know we may not be able to repair parts of degenerative tendons, there are still healthy spots. This is called treating the donut, where we focus on the donut (healthy parts), rather than the hole (degenerated parts). Although, more degenerative tendons may not have the capacity to progress to the above plyometrics.
External Pacing and Treating the Unaffected Side:
As mentioned earlier in the article, the central nervous is thought to be involved in tendinopathy. A strengthening program based on the principles above may be enough to return the tendon to normal, however alterations in biomechanics and neural activity can remain.
One way to address this is through external pacing. This has been shown to influence, and potentially rebalance the relationship between cortical inhibition and corticospinal excitability. Using a metronome to time repetitions to a set beat, or setting specific times for concentric and eccentric contractions is better than self pacing for altering neural activity.
Another way to treat this is by utilising the unaffected side in rehab. Not only should the unaffected side be treated as it is at risk of developing a reactive tendinopathy due to the loading changes, it can also impact the affected side. Specific exercises to a metronome on the unaffected side can help to normalise muscle activation and movement patterns on the affected side.
Treating the Chain:
Treating areas that are further up the chain may influence the amount of load going through a tendinopathy. For example, the calf, hip and hamstring may be treated in Achilles tendinopathy, or the shoulder and neck in elbow tendinopathies.
Heat and Ice:
Ice should only be used in the very acute stage as a pain management strategy. Regular use of ice for tendinopathy treatment is not beneficial for healing.
Heat can be used throughout rehabilitation, as it assists the tendon in preparing for load and activity. This can be done using heat cream or heat packs before exercise or activity.
Massage:
Massage directly over the tendon is not likely to be helpful, and could increase pain. However massage of the muscle belly, and areas further up the chain can be beneficial.
Dry Needling:
Dry needling is similar to massage, and is unlikely to be effective directly into the tendon. Dry needling surrounding muscles and areas further up the chain is useful for load management and symptom relief.
Ultrasound:
The benefits of Ultrasound for Tendinopathy treatment are not clear. Ultrasound may be beneficial in acute stages, when other options are too irritable. However, other treatment options are more effective.
Shockwave:
Shockwave can be an effective treatment option for less acute presentations. It is not a first line treatment, however can be helpful to compliment load management and strengthening if progress has started to plateau later in treatment.
Shockwave can kickstart the healing process and help with the realignment of collagen fibres.
Pharmacology:
Pharmacological interventions might be used in painful tendons as an attempt to reduce symptoms. Options such as Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), or injections such as Corticosteroids can be very effective at reducing pain in the short-term. However, outcomes in the medium to long-term for these interventions are not great.
Typically these interventions reduce pain, but they can mask the structural and loading issue that caused the tendinopathy in the first place. This will likely result in continuation of overloading the tissue, leading to the tendon moving further along the continuum.
Returning to Activity
Throughout rehabilitation of tendinopathy, we can slowly reintroduce aggravating activities as tolerated. It is very important that the tendon is able to handle the load it is given, and one way to monitor this is through the traffic light system.
The Traffic Light System
It is okay to experience some pain during activity with a Tendinopathy. However it is important that this pain does not become too high, and that it reduces once activity is finished. The Traffic Light System is an easy way to ensure pain levels do not mean any damage to the tendon.
The Traffic Light System uses the Visual Analogue Scale as a scale to score pain levels. This is a subjective scale, where pain is rated from 0-10, where 0 is no pain at all, and 10 is the worst pain imaginable.
The Traffic Light System works as follows:

- GREEN LIGHT = GO
- Pain scored < 3/10.
- Pain at this level is okay, and you can continue current activities.
- Pain scored < 3/10.
- YELOW LIGHT = CAUTION
- Pain scored 4/10 to 6/10.
- Pain at this level shoulder be monitored.
- It is okay to continue activity at this level, as long as it reduces to a green light (<3/10) following activity and the next morning.
- If pain stays as a yellow light, an appointment with your Physiotherapist is indicated and load should be reduced.
- Pain scored 4/10 to 6/10.
- RED LIGHT = STOP
- Pain scored >7/10
- Pain scored at this level means we should stop activity, as tendon load is too high.
- Load should be decreased, and an appointment with your Physiotherapist is indicated.
- Pain scored >7/10
Pain Diary
It is important to accurately keep track of our pain during and after activities when we are recovering from tendinopathies. Keeping a pain diary is a good way to track this. You can use the link below to access a pain diary.
Using a pain diary, we can also see trends in loading and pain. For example, pain gradually decreasing with the same activities, means the tendon is adapting to load correctly. Whereas pain gradually increasing with similar activities indicates the tendon may be becoming overloaded.
More Information
For information on specific common tendinopathies, see the links below to separate articles.
If you think you might have a tendinopathy, contact your Physiotherapist to assist in diagnosis and management.
References
Cook, J. L., & Purdam, C. R. (2009). Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. British Journal of Sports Medicine, 43(6), 409–416. https://doi.org/10.1136/bjsm.2008.051193
Cook, J. L., Rio, E., Purdam, C. R., & Docking, S. I. (2016). Revisiting the continuum model of tendon pathology: what is its merit in clinical practice and research? British Journal of Sports Medicine, 50(19), 1187–1191. https://doi.org/10.1136/bjsports-2015-095422
Cardoso, T. B., Pizzari, T., Kinsella, R., Hope, D., & Cook, J. L. (2019). Current trends in tendinopathy management. Best Practice & Research. Clinical Rheumatology, 33(1), 122–140. https://doi.org/10.1016/j.berh.2019.02.001
Rio, E., Kidgell, D., Moseley, G. L., Gaida, J., Docking, S., Purdam, C., & Cook, J. (2016). Tendon neuroplastic training: changing the way we think about tendon rehabilitation: a narrative review. British Journal of Sports Medicine, 50(4), 209–215. https://doi.org/10.1136/bjsports-2015-095215